Did testing and euthanasia protocols help create the appearance of a sudden-spreading deadly novel virus?
Did testing and euthanasia protocols help create the appearance of a sudden-spreading deadly novel virus?
The evidence gets stronger for those who care to look.
Some people were onto the midazolam / euthanasia story from very early on.
Although I was aware of the noise around Jacqui Deevoy’s one-hour 2021 documentary “A Good Death”1 as well as the data showing increased midazolam orders, it is to my chagrin that I didn’t pay enough attention to this story early enough, choosing to believe a variation of one of these singly or in combination:
The extra midazolam ordered in many places was not actually used, it was “just in case”.
The extra midazolam used was used for good reason, to ease distress and make the end of life more comfortable for those dying of covid.
However, I don’t believe either of those propositions anymore, largely because of the weight of evidence I have now seen, which amounts to strongly suggesting the following:
There is good evidence that more midazolam was ordered (and / or other drugs with equivalent modes of action)
There is good evidence that shortages of the drug (and related drugs) ensued
There are written protocols in existence which encourage its usage
These protocols are inappropriate and represent huge changes from established clinical practive for the treatment of respiratory infections
In the UK, midazolam usage is strongly correlated temporally to excess deaths, and the excess death curves are tightly synchronised across the UK in a pattern which is not consistent with pathogenic spread.
There were changes in laws in some places to facilitate its use where euthanasia had been previously illegal
There are disturbing eyewitness reports on various media AND also at Official Inquiries under oath, eg at the Scottish Inquiry
There is precedent for healthcare professionals being capable, in extreme circumstances, of carrying out what would ordinarily amount in law to homicide while thinking they are doing good. In this regard, I suggest reading this article which I wrote last year with Jessica Hockett
.
In summary, I believe the weight of the evidence suggests that the lives of large numbers of people worldwide were ended prematurely as a result of the administration of certain medication.
The way in which those directives came about is, at this time, unclear.
Was this an emergent event which was the result of some sort of societal mass delusional psychosis, one which involved the entirety of the healthcare profession buying into the story of the imminent arrival of a novel deadly virus, such that the application of these protocols was regarded as saving people doomed to die from a terrible death by “easing them on their way”?
Or was it part of a co-ordinated process by which a pandemic event was essentially staged?
I don’t know for sure at this point because we don’t have a smoking gun to show that there was co-ordination of the imposition of these protocols. What does seem clear, however, is that these actions did unnaturally create a sharp and steep uptick in deaths in many places around the world, all of which were categorised as “covid deaths”2. These death numbers would then have been the main source of the numerator in the reported infection fatality rates.
At this point it is worth reading this piece by Jessica Hockett
:

Was the sudden imposition of what can rather euphemistically be called “new protocols” causing this sharp and steep uptick in deaths (then blamed on “the virus”) the equivalent of the order to “sink the ships”? It certainly provided the magnitude and speed which is an essential part of a “shock and awe campaign”.
Now, onto some evidence. I have, over a period of some months, been collecting various articles and other sources pertinent to the above, and I have listed all these below. Some of these relate to intubation and ventilation policies which (in some places) are also intimately linked to the use of midazolam or similar drugs.
(The first half or so of the below are derived from this thread from 2020 on X by NellyTells
)
The list:
A link to a podcast interview with the veteran journalist John Helmer in which a change to French law legalising a euthanasia protocol is mentioned (around the 8 minute mark).
The link in the tweet no longer works but Nelly found the podcast on wayback machine, and I uploaded it here.
To quote:
…a presidential decree was issued more or less in secret on the 28th of March. It was published the day before yesterday in the online French news service Mediapart, in which it appears, that's the press report, the decree language is ambiguous, that doctors are being given an authority to use euthanasia drugs. What? Yes, although that's against French law.
A link to the next day’s edition to the same podcast (uploaded here) in which Pablo Ouziel (Spanish, associate fellow at the Centre for Global Studies at the University of Victoria) reports on a euthanasia protocol being applied to his father (around the 27 min mark).
To quote:
So my mother took my father to the hospital, to the local clinic, and they decided in the local clinic, the doctor decided to do an X-ray of my father's lungs. And they did the X-ray and the doctor said, OK, this is just pneumonia. It's not coronavirus.
And but he said, but please go to the next door, go to the hospital nearby so that they can do further checks. My father at that point refused. He said he was going home.
My mother as well. It's something that they've agreed to a long time ago that my father would not want to spend the last days of his life in a hospital. But anyway, so they went home and my mother said to the doctor, please remember to send us the oxygen machine.
So the next day, this is 10 days ago, she someone rings at their door and she thinks that it's the people coming with the with the machine. And it turns out that it isn't. It's two doctors dressed like astronauts coming into the house, telling my mother that my father has coronavirus and that he has 24 hours to live, that he's going to start coughing and that as soon as he starts coughing, my mother should start injecting him with morphine and a set of other things and do it continually every five hours until my father passes away.
Right. This is what was told my mother 10 days ago. My father yesterday was doing his accounting with me for four hours and today was, you know, basking in the sun in his garden.
And he's completely alive and kicking. And the doctors who are following protocol are actually were actually telling my mother to inject, you know, to put him to sleep in a country where euthanasia is prohibited. So it's very interesting what happens in the state of emergency.
A YouTube video of an episode of The Richie Allen Show in which a caller described how his mother in law…
This article in the UK’s Independent which described how:
The government is under pressure to go further on measures to relax rules on powerful painkillers such as morphine to prevent patients suffering “unnecessary pain and distress in the last days of their lives”.
On Tuesday the health secretary, Matt Hancock, announced staff in care homes and hospices would be allowed to “re-use” controlled drugs such as morphine and midazolam, with medication prescribed for one patient used for another where there is an immediate need.
But the Home Office today confirmed to The Independent that it had no plans to extend the rules to the care of patients in their own homes – a restriction experts and charities have warned could leave people suffering at the end of their lives.
Reading on, it is clear that the Royal College of General Practitioners wanted the same drugs to be made available for people at home, not just in care homes:
The Royal College of GPs (RCGP) welcomed the changes announced by Mr Hancock, calling them “a significant step forward”, but added: “This only applies to patients living in care home and hospice settings, so there is still work to be done to ensure patients living in their own homes have appropriate access to necessary medication in a timely way.”
This op-ed in RT regarding Swedish care homes which is quite confused. It seems to be critical of the “let it rip” policy on the surface, though also contains this:
To get an even clearer idea of what’s gone on, I interviewed Latifa Lofvenberg for a witness statement, which I shared on my Youtube channel. Latifa is a nurse who worked in a government-funded care home in Gavleborg, but is no longer employed there due to speaking out about what she witnessed.
She told of old people being left to choke to death for days on end, and of being instructed to administer morphine and a muscle relaxer, midazolam, which helps relieve anxiety while the patients slowly suffocate.
If an elderly patient eventually loses the fight with Covid-19, I believe it is far more humane to let them die of narcosis and carbon dioxide after we have done our best to save them, rather than resorting primarily to morphine and breathing complications, while denying them oxygen.
This article in The Daily Mail:
From that piece:
The number of prescriptions for a powerful sedative that can kill the frail doubled at the height of the coronavirus pandemic, raising fears it was used to control elderly residents in stretched care homes – or even to hasten their deaths.
Official figures show out-of-hospital prescribing of the drug midazolam increased by more than 100 per cent in April compared to previous months.
An anti-euthanasia campaigner last night said he suspected that the spike was evidence that many people had been put on end-of-life protocols or ‘pathways’.
The claims are unverified and were last night vigorously disputed by the Association for Palliative Medicine, which said that there were good reasons for the increase. Over the past five years, about 15,000 prescriptions for midazolam to be used outside of hospital have been written each month in England. In April, 38,582 prescriptions were made – more than twice the February figure.
Retired neurologist Professor Patrick Pullicino, who was instrumental in raising concerns a decade ago that the Liverpool Care Pathway was bringing forward patients’ deaths, believes the jump indicated something similar had happened. He said: ‘Midazolam depresses respiration and it hastens death. It changes end-of-life care into euthanasia.’
Prof Pullicino also claims that an official flow-chart intended to help health workers decide if people sick with Covid-19 were suitable for intensive care wrongly consigned those deemed too frail to end-of-life care.
That meant, he suggested, that some were not taken to hospital even though they could have been helped by doing so.
‘Certainly there have been more [unavoidable] deaths because of Covid-19,’ he claimed. ‘But to me this flow-chart encouraged use of end-of-life sedation with midazolam – effectively resulting in euthanasia pathways.’
This report about care homes in Australia in which the following was said to be happening:
Dr Robert Hoffman told the Australian that at Glenlyn Aged Care Facility, the Royal Melbourne Hospital had originally arranged to transfer patients at risk of “wandering” and infecting others to hospital, but then cancelled these plans. Instead, Dr Hoffman said, “Any COVID residents who were unwell were ordered as needed palliative care medications, morphine etc., one [resident was] as young as 46.” Some 15 patients and five staff have tested positive at the facility.
Around 1 hour 10 into this 2 April 2020 edition of The Richie Allen show a caller describes how the GP of his elderly frail mother-in-law wouldn’t go out to see her, but instead said they would “prescribe paracetamol and if that doesn't work I'll put an end-of-life package in place”. When the caller spoke to a contact at The Guardian he was told “we know this is going on…we can't get traction yet”.
This guideline from a “website managed by the IAHPC and is offered to the global palliative care community as a common shared space to do global advocacy for palliative care” specifies an insanely high dos of midazolam to relieve anxiety in patients “with covid”.
IAHPC is the International Association for Hospice and Palliative Care. They describe their mission thus:
We serve as a global platform to inspire, inform and empower individuals, governments and organizations to increase access and optimize the practice of palliative care.
From that guideline:

The dose suggested there - for restlessness and anxiety - is huge, translating to 120 to 240 mg in a 24 hour period.
The maximum dose I could find anywhere for end of life was 60 mg / 24 hours, with most suggesting doses in the region of 10 to 20 mg per 24 hour period.
The above guideline was described further at this webinar given by the Worldwide Hospice Palliative Care Alliance which describes itself thus:
With our organisational members in over 100 countries, we provide a global voice on hospice and palliative care
The Worldwide Hospice Palliative Care Alliance (WHPCA) is an international non-governmental organisation focusing exclusively on hospice and palliative care development worldwide. We are a network of national and regional hospice and palliative care organisations and affiliate organisations.
Some of their other material (all listed here) is eye-opening. I was particularly struck by this video (only 4 mins long), from Ryan Pferdehirt of the Kansas-based Center for Practical Bioethics:
Note the willingness with which it was suggested that the rights of the individual be subjugated to “the greater good”, which seems a somewhat Orwellian version of their stated vision, which is “that ethical discourse and action advance the health and dignity of all persons”.

Could that be linked to this story? One has to ask, since the disabled obviously make up a much smaller fraction of the general population than 60%, and there would be no reason why many or most disabled would be more susceptible to a respiratory virus than an able-bodied person anyway.

This Washington Post article was published on 25 Mar 2020:

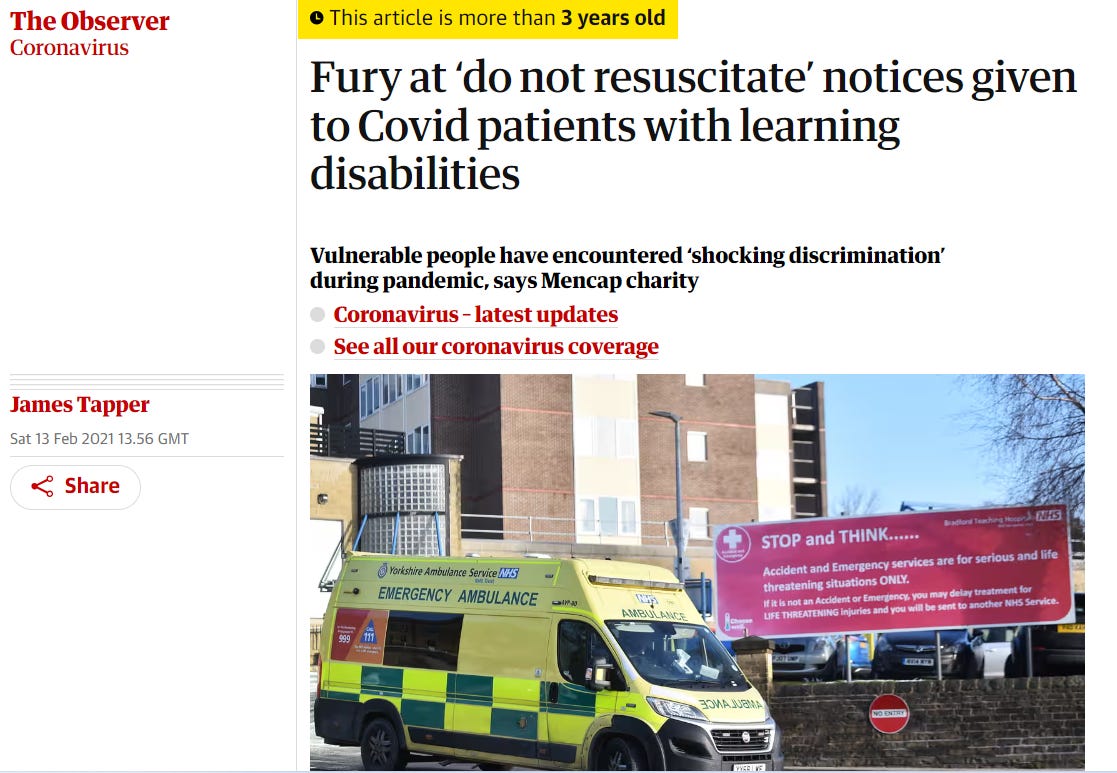
It seems that the DNR policies went as far as those with “learning difficulties”, according to this Observer article.


Here’s my recent piece which suggests that it's naive to think DNRs are only relevent to cardiac arrest situations. As John Campbell says in this video I cited, a DNR will inevitably be interpreted as “put on end of life pathway:
..many nurses interpret Do Not Attempt Resuscitation orders as well….basically we've gone on to palliative care, we've basically given up on saving this patient's life; this is completely wrong but this is the way it's often interpreted.
In the UK, NICE, a body responsible for writing clinical guidelines, issued the notorious NG163 - end of life guidelines for covid patients - which appeared to simply mirror the advice appropriate for true end-of-life situations to “covid patients”.
Andrew Bridgen went through the history of this guideline in a speech in Parliament on 18 April 2024 - see here for a transcript and a link to the video of the speech.
Notably, he states that:
They sent people home and told them to take paracetamol until their lips turned blue.
Then they sedated them, put them on ventilators and watched them die.
It gets worse, the protocol was a binary choice between two treatment tracks. Once admitted, ill patients were either to be ventilated in intensive care or, if they were not fit for that level of care, they were to be given end-of-life medication including Midazolam and Morphine.
The body responsible for this protocol - NG163 which was published on 3rd April 2020 - is called the National Institute for Health and Care Excellence – NICE.
Giving Midazolam and Morphine to people dying of cancer is reasonable but they have a side effect. The side effect is that these drugs have a respiratory depressant effect.
It is hard to imagine a more stupid idea than to give people struggling to breathe, drugs that do that. Yet that’s what they did.
Why was the warning letter regarding the use of Midazolam in NICE guideline NG163 to the British Medical Journal on 19th May 2020 signed by two Professors and nine Doctors ignored? Especially as it would seem it’s a replica of Abolished Liverpool Care Pathway in dosages and combined use of Midazolam plus an opioid.
NG163 stated that a blanket start dose of 2.5 mg of Midazolam should be injected regardless of age, body weight and comorbidities, how can this be medically acceptable as results show titration was not possible at such a dose for many elderly and who authorised it?
Why was Midazolam then removed from the same updated guideline NG191 on 30th November 2023? (As it was removed is it now considered and admitted it was a mistake to ignore the warning of the inclusion of that specific drug in NG163)?
It’s now been confirmed by subsequent letters from Ministers to families that doctors and nurses should have treated the individual patient with their own knowledge rather than strictly follow NICE guideline NG163 (as suggested by Quince and Stephenson) so if the warning letter from 11 experts to the BMJ was correct is the blame with NICE, NHS England or individual doctors and nurses, should legal action find verdicts of unlawful killing?
I would like to pay tribute to the Scottish Covid Inquiry which is hearing extensive, heartbreaking evidence of the effect of this alternative protocol on real people, real lives and sadly real and unnecessary deaths. People scared. People angry. People dying. People gasping for their lives away who might have been saved.
I very much hope that the eventual Scottish Inquiry Report addresses in detail the NICE decision making on the alternative protocols for those with Covid.
All these deaths were ascribed by the government to covid as if no other factors needed to be investigated.
But this is one example of a scandal that if it wasn't for the Scottish Inquiry would never be investigated and never learned from.
Anyone who raised this problem during the pandemic was smeared as a covid denier.
Even worse
NICE has now removed these alternative protocols from its website. All other old protocols are still there for historical reference.
Why have NICE removed this protocol from their website? Are they ashamed of the harm they caused?
They certainly should be.
I have mentioned the Scottish Covid Inquiry several times. Here’s an overview of how this Inquiry differs from the London version.
I also highly recommend all of Dave’s posts here; ones are most pertinent to the subject being discussed here are these:

Here’s a tweet (from biologyphenom’s X account) linking to a video about someone being pressured into having a DNR order put in place.
An Australian investment analyst called Wilson Sy recently published paper this paper in which he studies the relationship between excess death and extra midazolam doses used (over expected levels). Here is the abstract:
Macro-data during the COVID-19 pandemic in the United Kingdom (UK) are shown to have significant data anomalies and inconsistencies with existing explanations. This paper shows that the UK spike in deaths, wrongly attributed to COVID-19 in April 2020, was not due to SARS-CoV-2 virus, which was largely absent, but was due to the widespread use of Midazolam injections which were statistically very highly correlated (coefficient over 90 percent) with excess deaths in all regions of England during 2020. Importantly, excess deaths remained elevated following mass vaccination in 2021, but were statistically uncorrelated to COVID injections, while remaining significantly correlated to Midazolam injections. The widespread and persistent use of Midazolam in UK suggests a possible policy of systemic euthanasia. Unlike Australia, where assessing the statistical impact of COVID injections on excess deaths is relatively straightforward, UK excess deaths were closely associated with the use of Midazolam and other medical intervention. The iatrogenic pandemic in the UK was caused by euthanasia deaths from Midazolam and also, likely caused by COVID injections, but their relative impacts are difficult to measure from the data, due to causal proximity of euthanasia. Global investigations of COVID-19 epidemiology, based only on the relative impacts of COVID disease and vaccination, may be inaccurate, due to the neglect of significant confounding factors in some countries.
This substack article reviews the paper. Notwithstanding that the paper is open to criticism, the findings, together with the other circumstantial evidence provided here, at least raise a hypothesis which requires further investigation, rather than the outright suppression of the story which we have seen.
As I tweeted here, a Dr. Richard Levitan was quoted in this NYT article published 14 April 2020 as saying:
“Never in my life have I had to ask a patient to get off the telephone because it was time to put in a breathing tube,”
Needless to say, certain drugs - including Midazolam - are in regular use for intubation. Recall that it is estimated that 90% of ventilated patients died.
I believe doctors like Dr Levitan - who deleted his twitter account (@airwaycam) - will, look back at their part in the events of 2020 with a mixture of embarrassment, denial and shame3.
With no apparent regard for the significance of anything said in the article, the byline to the NYT article above, by the way, was:
"Ironclad emergency medical practices — about when to use ventilators, for example — have dissolved almost overnight."
The Guardian published possibly the most sinister article I have seen during the entirety of the past 4 years.

To quote:
Death penalty states in the US are stockpiling medicines for lethal injections that could save the lives of hundreds of coronavirus patients were they released for medical use.
A group of prominent medical practitioners and experts has issued an appeal to capital punishment states to release their stocks of essential sedatives and paralytics that they hoard for executions. The drugs are among the most sought after in hospital intensive care units around the country where shortages of the key medicines are putting lives of Covid-19 patients at risk.
This article in the New Yorker contains the following account of the death of NYC’s first “coronavirus victim”. Again, the theme is intubation of patients who are well enough to talk, ignoring the overall signs and symptoms and religiously following a protocol and a series of test results.
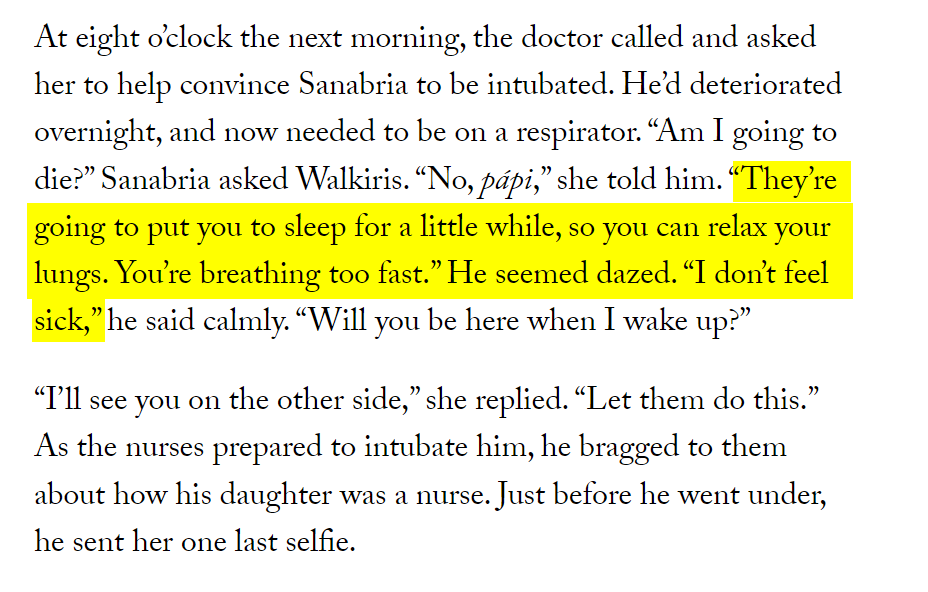
From this piece in New York magazine:

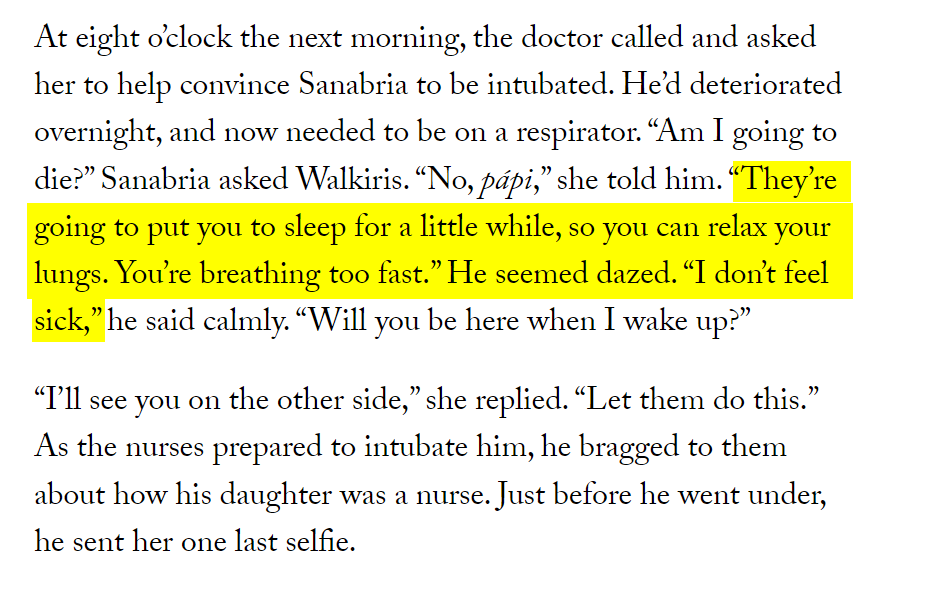
"Early on, doctors were sometimes intubating patients when their blood-oxygen readings seemed to indicate they were about to crash, even if they were still wide awake and talking. But one of the unusual effects of COVID was that patients seemed able to tolerate alarmingly low blood-oxygen levels—numbers that would normally prompt intubation—while the stiffness of their lungs made pushing air in via the mechanical ventilators much more difficult, like trying to inflate a steel balloon. For these patients, “taking away their respiration and awareness and homeostasis was actually more harmful than anything,” says Burmon."
Back to the Scottish Inquiry. In the below video John Campbell covers the evidence given by Adam Stachura, Head of Policy and Communications with the charity Age Scotland.
His written Witness Statement can be found here. The whole thing is worth reading in full. Amogst other things he states:
From the end of March and through April we were getting a significant number of calls from people saying they have been contacted, out of the blue by their GP, or sometimes it was the practise reception staff, asking if they would agree to having a DNACPR4 decision on their medical records.
This wasn't restricted to March and April. As an example, somebody got in touch with us later on in 2020 who was concerned about their grandfather who a veteran. He was over 100 years old and who still lived independently, on his own. We understand from this exchange that paramedics arrived at his door one day and they handed him a bit of paper and said, "you need to keep this by your bed". It was a DNACPR decision document or slip. A photo was taken and sent to us by email, and I remember seeing it.The slip was signed by a clinician that said discussion had been had with patient and reason was just two words "communication difficulties". Presumably, linked to his hearing loss.
From our discussions with other organisations such as Scottish Care as I recall, from media reports and calls to our helpline we had a sense that this was also be happening in care homes, where all residents were having DNACPR decisions issued in a blanket manner, not on an individual basis.
We also found examples of people who upon leaving hospital found DNACPR decisions in their discharge papers without any discussion having been had with them. The box was ticked which said they had had a discussion, where in fact none was.
From my own article on midazolam usage in Italy, citing B Braun’s5 website.
On the morning of March 21, 2020, a delivery vehicle out of Melsungen, Germany, arrived at the warehouse in Mirandola. It was a Saturday, and normally there were no deliveries on weekends. In these times, though, nothing was normal. The vehicle was carrying 10,000 doses of the sedative midazolam, which was urgently needed in Italy for the mechanical ventilation of thousands of COVID-19 patients who needed help breathing. Gabriele Ceratti worked with the italian team in Milano and Mirandola to make the delivery possible in just a few days.
Mr. Ceratti, what challenges did you face when procuring the sedative?
Due to the extremely critical situation, the hospitals suddenly needed three or four times the normal amount of this drug. We knew that we would have to get it from another country, but to do that we first needed a special permit - the vials of midazolam from Melsungen had labels in German and English, but only labels in Italian are allowed here.
Why did you and your team decide to take on this responsibility?
In those awful days of the first wave, we saw how the hospitals were in desperate need and we knew right away that we had to respond. Even though we got the ball rolling, it never would have worked without the Regulatory Affairs people at B. Braun in Italy and Germany. They, too, immediately took responsibility and acted. This kind of permit normally takes weeks, but we got it in just a few days. It was an extraordinary situation.
How did you get through that difficult time?
It’s the result of having a great team at B. Braun - both here and in Germany. We could feel the support of our German colleagues quite a lot. Everyone was so kind and sensitive, they understood it was time to respond immediately in order to help Italy and all the patients in this terrible situation.
What gives you hope?
The emergency procurement of midazolam was the first time, but certainly not the last time in this crisis, that we were able to help quickly. We were able to do something similar with the sedative propofol and pumps for hospital beds.
I could go on, but won’t for now. There is basically unlimited evidence out there for those who choose to look for it, and at times it can be overwhelming. But you get the picture.
With thanks also to Jessica Hockett for some of the above links.
This, of course, would have also created a positive feed-back loop of fear and the perception of how “deadly” “the virus” was.
Do not attempt cardio-pulmonary resuscitation.
A European medical products distributor.
Source: Jonathan's Substack


Comments
Post a Comment