Why do people still believe in covid?
Why do people still believe in covid?
Three keys to understanding why there was no pandemic

Sure, PCR was done badly but there was a novel virus, right?
In the early period of the covid event much of the reporting of the gross inadequacies of PCR testing was almost entirely focused on one narrow technical issue - whether the cycle threshold (CT) used to declare a PCR positive for SARS-CoV-2 was ‘too high’.
Excepting those who ascribe to the ‘no virus’ theory, this focus on excessive CT was myopic and excluded wider issues related to PCR. For instance, these two reports may have summarised the already well documented problems with CT, but they didn’t reflect on a number of wider issues we will discuss in this article:
Collateral Global (Jefferson, Dietrich, Brassey and Heneghan, February 2022)
The UnderDog (March 2023)
High CT values were used to determine infectiousness, asymptomatic versus symptomatic infection, viral load, viral shedding and clinical severity. Likewise, at a population level they were used to define ‘genuine’ cases for the purpose of epidemiological tracking of virus prevalence.
Here are some quotes from the Collateral Global report that give you some idea of how CT framed the discussion:
The smaller the quantity of (targeted) genetic material present in the test sample, the harder the PCR must work to find it, i.e., the more cycles of amplification it has to perform. The technique becomes more sensitive as the number of amplification cycles is increased until it’s searching for a needle in a haystack. The Ct is set by the laboratory or test programme, and as Ct is raised, the likelihood of a positive test result will increase for a given sample.
The UK Health Security Agency guidance reports, "samples with Ct<25 are considered to have a high amount of virus, those with Ct>25<30 are considered to have a medium amount of virus, and those with Ct>30 are considered to have a low amount of virus."' Therefore, when the Ct is set at 45, the test can detect single gene fragments and render these as a positive result even though gene fragments themselves are not infectious and can linger in the patient long after the infection has passed.
However, PCR alone cannot differentiate between the presence of whole viruses (which can be transmitted and infect individuals) and small fragments of genetic material that are not infectious. The shedding of this viral debris can occur over a prolonged period of time.
Notice how the discussion does not cast any real doubt on ‘what’ is being detected, either properly or improperly. Small fragments of genetic material and ‘virus’ are all implied as synonymous with a new novel deadly virus - SARS-CoV-2. Logically therefore genuine infections, confirmed by low CT, must exist and therefore there can be no doubt that SARS-CoV-2 existed and was causing these infections, and PCR could reliably confirm this. High CT cast no doubt on the presence of the virus but simply questioned whether the infection was active or not or perhaps had ‘fragmented’, hence whatever the result, the test was apparently confirming the fact that the individual tested was at some point on the infection ‘life cycle’.
The debate around PCR then settled into two camps pursuing a false dichotomy:
The Covidians - “the tests are not sensitive enough”: they are missing active SARS-CoV-2 infections, therefore we need higher CT.
The Dissenters - “the tests are too sensitive”: they are picking up fragments of inactive SARS-CoV-2, therefore we need lower CT.
This debate spilled over into social media where everyone commenting on PCR did so by repeating these two dichotomous issues with PCR tests. Likewise, hundreds of FOI requests were written to extract admissions from health authorities, across the globe, forcing them to reveal they were using high CT values to diagnose SARS-CoV-2 infection. When the authorities confirmed this (they were, of course, using high CT levels) the response was ‘Gotcha!'
We initially fell victim to this myopia, believing in 2020 and into 2021 that PCR must be, in principle, diagnostically accurate in the sense that (other than when there is inadequate practice or poor-quality equipment) false positives for SARS-CoV-2 were mainly the result of CT thresholds being set ‘too high’. Here is a, non-exhaustive, list of articles we wrote that entirely depended on determining false positive rates based on case reporting (itself obviously based on PCR) (false positives, limits, 1 in 3). In all of these we were explicitly arguing, based on the data and evidence available, that these problems led to the artificial inflation of cases (which they did), but failed to identify, what we subsequently discovered, was the primary root cause driving this inflation of case numbers.
There was little to no suppression of the discussion of high CT on twitter and throughout ‘covid dissident’ circles, and any technical analysis of PCR ‘worth its chops’ would discuss excessive CT values in great detail to the exclusion of much else.
Was this a limited hangout?
Was discussion of the problem with CT permitted, or even perhaps actively encouraged to confirm in everyone’s minds the existence of a uniquely deadly and novel pathogen that could be detected by PCR? Or if not, amounting to intentional misdirection, did this arise by social contagion or psychological self-deceit?
Notwithstanding the widely distributed video of PCR inventor Carry Mullis warning about inevitable false positives from CT values set too high, it is remarkable how so many people jumped on the same issue at the same time.
PCR positive for anything and everything?
So, what else was going on with PCR that ‘they’ didn’t want you to know or that you deceived yourself into believing? (if you subscribe to Desmet’s ‘mass formation’ theory).
By definition, and in an idealised context, whether or not a positive PCR test result is ‘correct’ depends on whether the virus is actually either present or absent. So, if the virus is ‘absent’ but the test result is positive we have a false positive and if the virus is ‘present’ and the test result is positive we have a true positive. If the true negative rate is low, the test is said to be highly specific and if the true positive rate is high, the test is said to be highly sensitive.
As we have said, given the PCR test result was said to depend on how much virus or how many viral fragments are present on the swab taken, a positive result on 45 cycles might be explained away as someone recovering from the virus, or in the early phase of infection rather than genuinely infected or infectious at the time of the test.
But notice that the whole discussion of the meaning of the false positive result, along with ‘you are somewhere on this infection life cycle’ remains laser focused on ‘infection by this, and only this, novel deadly virus’.
In an ecosystem which we share with a huge number of (known and unknown) viruses classifying one specific virus as either present or absent is a pretty stark binary choice. While everyone was talking about false positives due to high CT thresholds what was not being discussed was whether the PCR test for SARS-CoV-2 might have been detecting other viruses, known or unknown.
So, actually the most relevant question was not the CT value used in the test, but how specific was the test to the virus, known as SARS-CoV-2, and might that test have been flashing positive in the presence of other viruses or other substances? To put it another way - was the PCR designed to cross-react with other viruses? This question is critical to understanding the nature of the covid event.
We were warned very early on by way of the Corman-Drosten report that the SARS-CoV-2 PCR test was flawed (pre-print submitted to Eurosurveillance, and rejected, available here):
a design relying merely on close genetic relatives does not fulfill the aim for a “robust diagnostic test” as cross reactivity and therefore false-positive results will inevitably occur.
However, in our experience all discussion of these questions in private discussion groups, with supposedly highly qualified experts in PCR, was deemed verboten, and dismissed as either irrelevant or scientifically illiterate. Many of these ‘experts’ claimed that, with a suitably chosen CT value PCR testing was confirmed the presence of the novel virus. Others flip-flopped on the issue over time.
Here we explained why these arguments were wrong, and that the PCR test was not specific to SARS-CoV-2. In this article we described our conversations with another well-known PCR expert, who still believes that PCR testing validated people’s covid morbidity experiences (they got ill) and given this they would never be dissuaded from the belief there was a pandemic.
We broke the story of another major scandal about PCR testing in 2021, which was much ignored at the time and still is. In it we reported:
We have recently discovered that UK laboratories have been routinely recording a significant proportion of Covid-19 test results as positive based on the presence of one target gene alone, when there should have been two or more, as required to comply with WHO rules and manufacturer instructions.
What we had discovered showed that PCR testing did not only just suffer from the excessive CT scam, but that the testing itself was almost entirely arbitrary. The PCR test applied were actually testing a single genetic characteristic of the SARS-CoV-2 virus rather than two or more as required, and one that might be similar to those present in other viruses.
This discovery should have set alarm bells off in the covid dissident movement, but it failed to get any traction. Unfortunately, it took us too long to work out why it did not.
If the PCR test was non-specific to SARS-CoV-2 then what was it cross-reacting to? What was causing the tests to come up positive?
The Three Keys

To our minds there are three key findings that sum up everything you really need to know about the scam of PCR testing. Few people talk about these key findings mainly because they still ‘believe in covid’, but when considered as a totality they should persuade even the most casual reader that there was never a pandemic caused by a deadly novel virus spreading around the globe.
Key One - Disappearing flu (and other viruses)
We’ve written extensively on the disappearing flu and the absence of other viruses during the early period of the covid event. The global downward trend in the reporting of competing bacterial and viral infections during spring 2020 is illustrated by this chart, published by the BioFire syndromic trends reporting system, showing the percentage detection rate of pathogens in the USA from 2019 through to 2021.
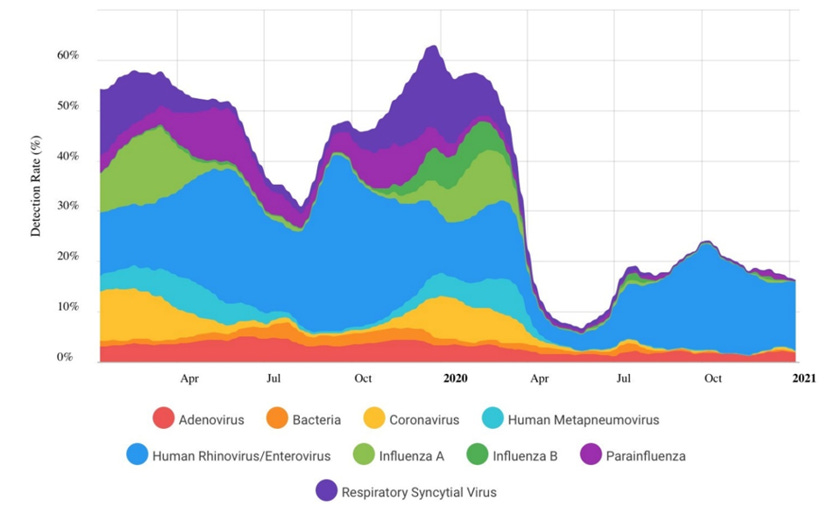
Where did all of the other viruses and pathogens go?
Short answer- the flu (and other viruses) didn’t actually disappear we simply stopped looking for them. It is almost as if the king of the colds - flu - had been deposed and replaced by the usurper - SARS-CoV-2 - who could wear the corona crown during the ‘pandemic’.
Key Two - A lie in plain sight
In 2020 Etievant et al published a paper analysing the performance of WHO referral laboratories in testing PCR assays for SARS-CoV-2. The laboratories evaluated included Charité (Germany), HKU (Hong Kong), China CDC (China), US CDC (United States), and Institut Pasteur, Paris (France).
They performed specificity testing for other respiratory viruses: human coronaviruses 229E, OC43, HKU1, and NL63, human influenza A and B viruses, rhinovirus, respiratory syncytial virus, parainfluenza virus, adenovirus, metapneumovirus, and picornavirus.
No false-positive results were obtained on clinical samples that tested negative for SARS-CoV-2 and/or positive for viruses other than SARS-CoV-2, except for gene E for Berlin Charité, Germany, and gene N2 for the US CDC, which were positive for all specimens and replicates, including negative samples and controls (including water!)
To view the test results you need to look at the supplementary materials from which the below table is reproduced. The left-hand column lists samples negative for SARS-CoV-2, some with competing viruses present and others with human tissue or water. These were all used to challenge the PCR assays formulated by each WHO referral laboratory. The row under the laboratory name lists the genes used by their assay to determine a positive result, with ‘ND’ meaning not detected (i.e. negative) and a value meaning a false positive detection at that numeric cycle threshold.
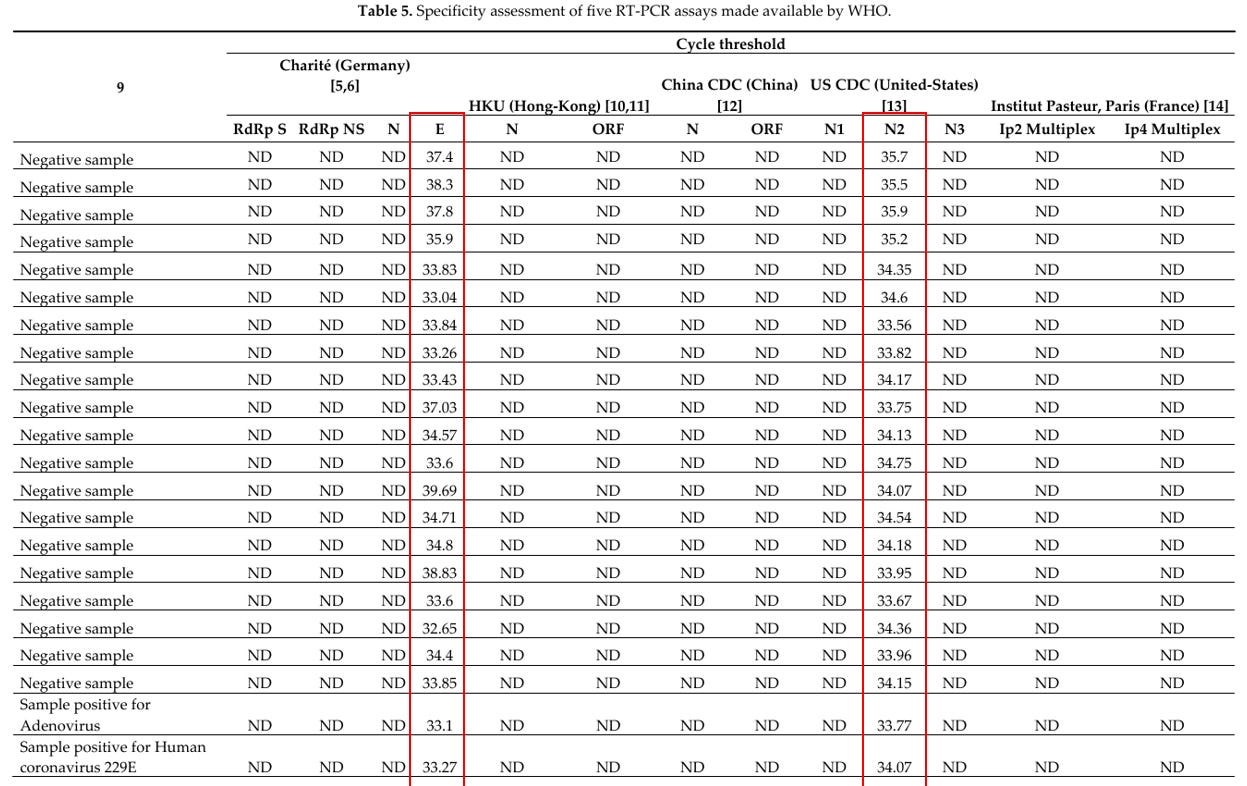
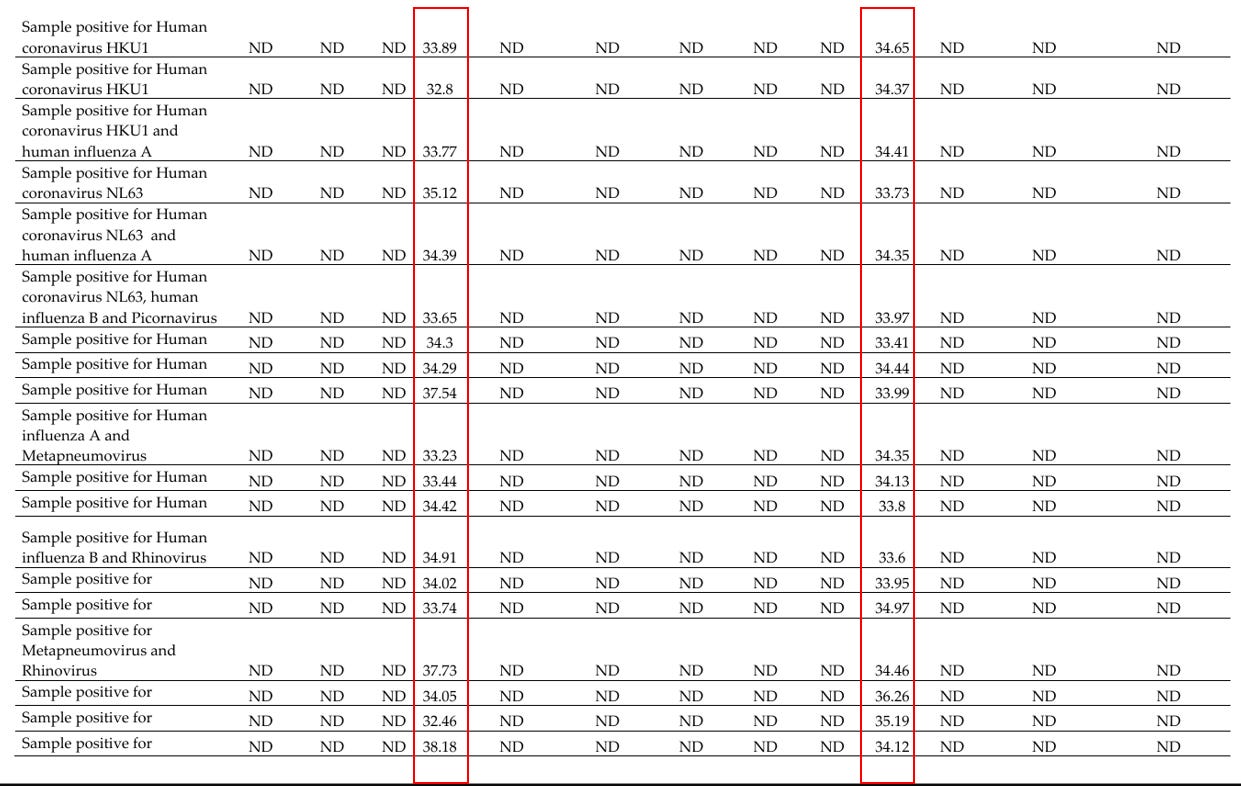
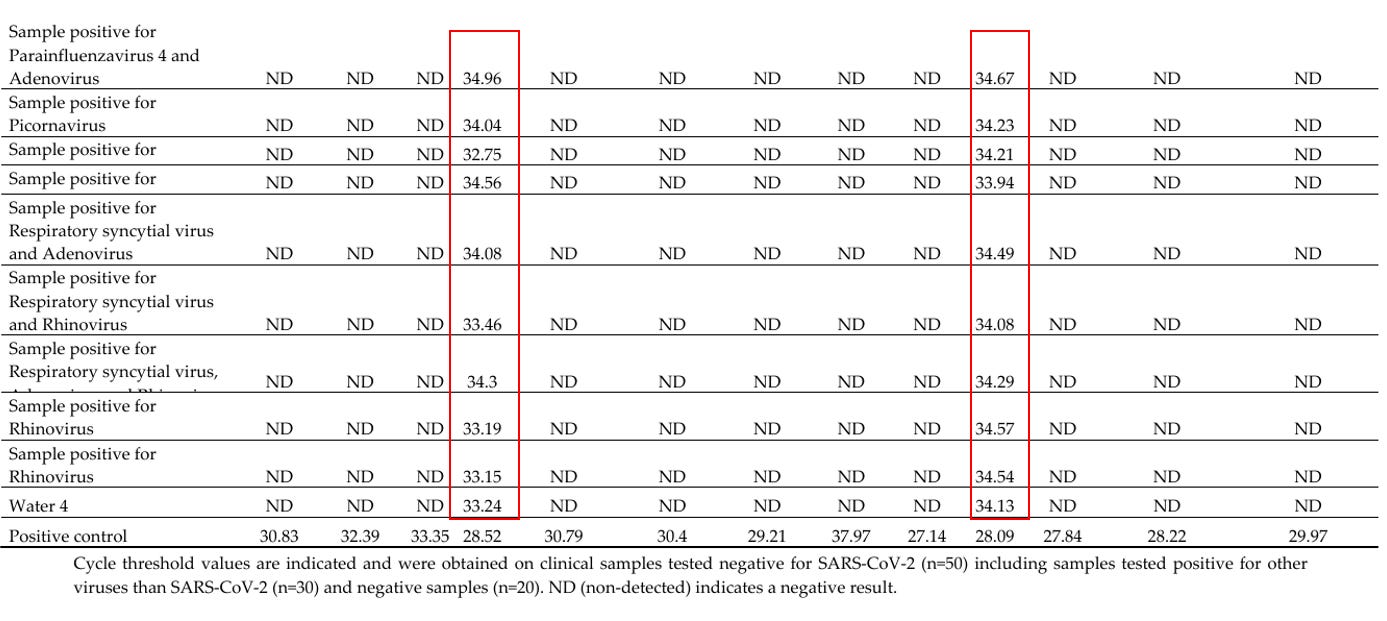
Here we have the best laboratories in the world supervised by the most competent regulators and populated by the most qualified scientists, who have managed to produce PCR tests that give 100% false positives using samples of influenza, the common cold, human tissue and water. Notice that all of these samples would be reported as 100% positive on only one target gene, exactly as we reported was happening in the UK in 2020/21.
In a podcast interview [19] on March 18, 2020, Christian Drosten, head of virology at Berlin Charité, Germany, discussed his PCR test and said (in translation):
We are only testing the new coronavirus in humans with this test. If we test a patient sample and it is positive, then it is this new coronavirus and in no case one of the known other coronaviruses.
Surely, the covid dissident movement should have been ‘all over this’. We only stumbled across the Etievant et al paper in 2024, but it is hard to imagine such an important study being missed by absolutely everyone up until that date, and it continues to be ignored since. No one has raised an eyebrow at Drosten’s assertion that this test detected the novel virus and that alone, yet we have a peer-reviewed paper showing the PCR test designed at his own institution was obviously flawed.
It should also be pointed out that the issues described above in relation to cross-reactivity of the testing with other viruses or other substances would act synergistically - and powerfully so - with any physical cross-contamination caused by sub-par lab handling techniques, which were widely reported and inevitable given the speed of rollout.
There was nothing ‘new’.
Key Three - Lack of novel symptoms
The final key is the fact that there is a lack of any clear symptoms of this new disease caused by the supposedly novel pathogen. We reported on this here. The symptoms of covid are indistinguishable clinically from those which a clinician would associate with a ‘flu’ or a ‘nasty cold’, pre-2020.
Furthermore, it was already well known that objective confirmation that a particular virus is causing respiratory illness symptoms cannot be done by PCR test. This is because of the inability of swabs to reliably collect and identify causative agents.
That was the (as yet unchallenged) conclusion of the pivotal CDC EPIC study in two 2015 NEJM articles - one done on adults and one on children. Hence a positive result gained from a sample taken from the upper throat or the nose does not mean an infection in the lung is caused by the detected pathogen. Just because a patient is PCR positive (from a nasopharyngeal swab), we cannot conclude the symptoms were caused by whatever virus was tested for!
Thus, any clinical discussion about infectivity is essentially moot and the fundamental basis for using PCR to track virus spread, morbidity and mortality is a sham.
Of course, as described here, because of the multiplicity of viruses associated with ‘influenza like illnesses’, the ‘disappearing flu’ trope - accounted for by the true believers by the phenomenon of viral competition (for which no evidence actually exists as we wrote here) - would require such competition to miraculously act upon a wide range of such possible causative agents, not just influenza.
Why is this still being ignored?
Similar to lab leak versus wet market, in 2020 we were presented with another false dichotomy about PCR tests and invited to take one of two sides - the tests are too sensitive, or they are not sensitive enough, but either way each option is framed on the supposition that a novel pathogen is in circulation. Discussion of the third option - that the tests were not picking up a new novel virus at all but were repackaging other viruses and presenting them as novel were ridiculed, ignored, suppressed and censored.
Why is this evidence still being ignored five years after the initiation of the event?
Why do people still believe in covid?
Source: Where are the numbers?


Comments
Post a Comment