"A Half Truth is a Whole Lie": The Omicron Variant, Cross-Reactive Immunity, and the Manufactured Illusion of an Unprecedented Virus
"A Half Truth is a Whole Lie": The Omicron Variant, Cross-Reactive Immunity, and the Manufactured Illusion of an Unprecedented Virus
Meanwhile, another study published in medRxiv (preprint) on December 8th, 2021, confirmed that vaccine-escape is happening with the Omicron variant, which means that the current batch of vaccines are not capable of neutralizing the Omicron variant. Too bad for everyone that's already had 3 doses of the magic elixir. Go back to square one.
There are moments when the public health messaging during Covid reminds me of the well-known parable of the blind men and the elephant wherein the blind men argue about the nature of an elephant based on the kernel of truth at their fingertips despite being utterly unable to see the larger reality standing before their eyes. But we are not living through a harmless parable. Our public health officials, vaccine makers, and media are manipulating our perception of reality. They are trying to blind us from seeing the full elephant by using deliberate oversimplification, half-truths, and out-of-context facts to manufacture (and exploit) an illusion of unprecedented danger. The most damaging lies are the ones that are built on a distortion of the truth.
So, it's time for another deep dive into the evolution of variants and the subtleties of our immune systems to get some perspective...
"A half truth is a whole lie." — Yiddish Proverb
 |
| Figure 1: The Blind Men and the Elephant: oversimplification conceals the broader picture. But unlike the blind men in the parable, the half truths told during Covid are being told by those whose eyes are wide open to the whole lie but want to prevent you from seeing the whole elephant. |
Table of Contents
Unravelling the Contradictions: How Can Natural Immunity Be Long-Lasting and Still Not Protect You Against Next Year's Variant?
Let's imagine you got infected by the original Wuhan strain of the SARS-CoV-2 virus. Your immune system has now been trained to give you natural immunity... to the original Wuhan strain. The current batch of vaccines are likewise based on this Wuhan strain. The Alpha variant is genetically very similar, so your immune system will also recognize and neutralize the Alpha variant. But as mutations stack up, it becomes harder and harder for your immune system to recognize and neutralize new variants as they become increasingly genetically distinct from the variant that infected you. You may still have long lasting immunity to the Alpha variant, but perhaps only partial cross-reactive immunity to the Lambda variant, and so on. The further new variants drift from the genetics of the variant you catch, the less efficient your adaptive immune response will be in neutralizing these new variants.
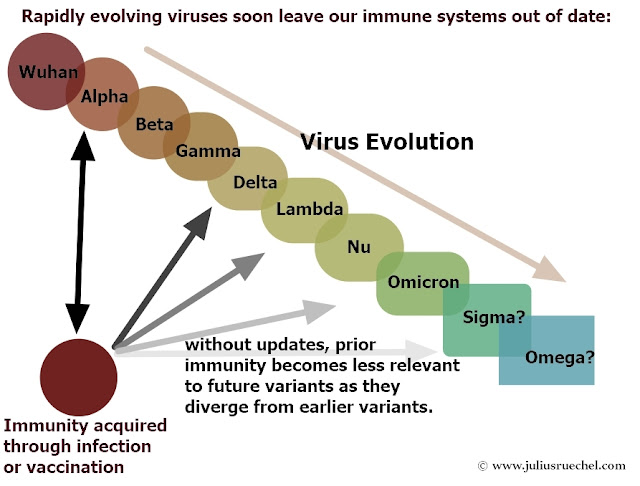 |
| Figure 2: Prior immunity becomes less and less effective as new variants evolve. |
Note, this is a separate and compounding issue to the gradual fading of immunity, which I discussed in my recent book, Autopsy of a Pandemic #CommissionsEarned. So, to be clear, there are two separate issues that affect our immune system's ability to protect us against re-infection: 1) fading immunity as the adaptive immune system gradually forgets its training and 2) the issue of genetic drift, which eventually allows newly emerging variants to bypass our immunity even if we still have immunity to a previous variant.
With a fast-mutating virus like a coronavirus, it was always just a matter of time until some new variant would be able to start re-infecting people even if they acquired long-lasting immunity through a previous infection (or through vaccination - more on that boondoggle in a moment). It's called immune escape. So, beyond a certain point, long-lasting immunity doesn't matter because the virus has moved on from what your immune system has been trained to do. The only way to prevent our immune systems from being left behind by the never-ending conveyor belt of new variants is to periodically update our adaptive immune systems to recognize changes to the evolving virus. And no, this is NOT a case for a lifetime regimen of booster shots, as you will soon see.
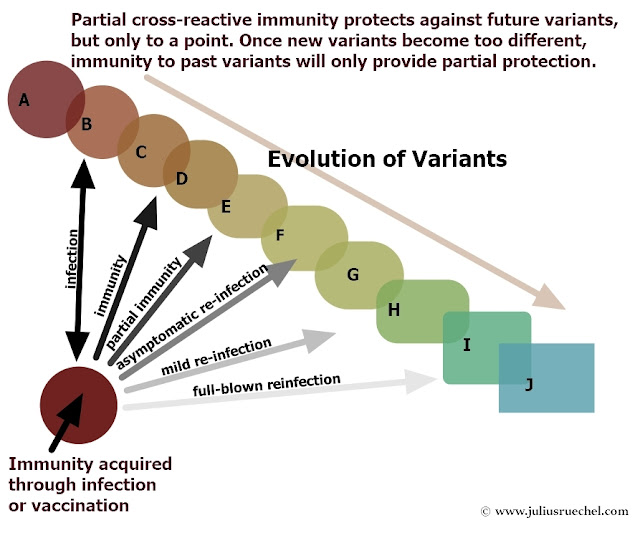 |
| Figure 3: Your adaptive immune system is trained to recognize and neutralize the particular variant to which you are exposed. New variants will eventually be able to get around it unless your immune system is periodically updated to recognize the changing virus. |
With enough time and without updates, immune escape will happen with ALL viruses, including viruses that have much slower genetic drift. It's just that a slowly evolving virus like measles might take a lifetime, or longer, to accumulate enough mutations to start to escape the protection of your natural (or vaccine-induced) immunity. But if you could extend your life by a few extra centuries, even if your immunity to measles never fades, the ever-evolving measles virus would eventually be able to re-infect you unless your adaptive immune system is periodically updated to recognize new variants before new variants become too unfamiliar.
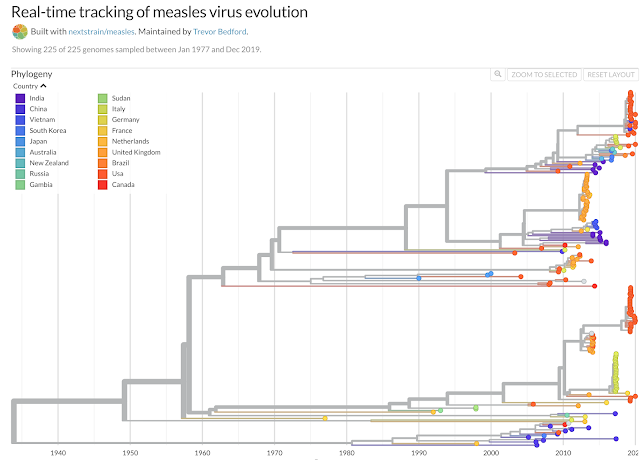
The following chart shows how much the genetics of the measles virus have changed (and diversified) from the variant circulating in the 1930s. No virus remains unchanged as time passes by. As long as a virus exists, the mutations never stop.
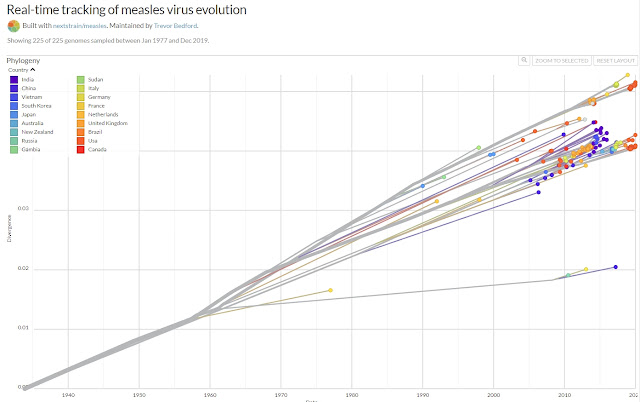 |
| Figure 4: Measles virus over time, showing how much its genetics have diverged (and diversified) from the variant circulating in the 1930s. (Source: nextstrain) |
And this chart of the measles family tree shows all the genetic branches that have evolved since the 1930s:
 |
| Figure 5: The measles family tree (phylogenetic tree) shows all the genetic branches of measles that have evolved since the 1930s. (Source: nextstrain) |
For context, here is a chart of the much more rapidly evolving influenza A/ H3N2 family tree showing all the genetic branches that have evolved in only the last 6 years. Virus evolution is relentless and perfectly normal, it's just that prior to Covid, conversations about variants rarely made the 6 o'clock news. We are human — we fear the unfamiliar. Cue the malicious new vocabulary of Covid: "variants of concern".👀
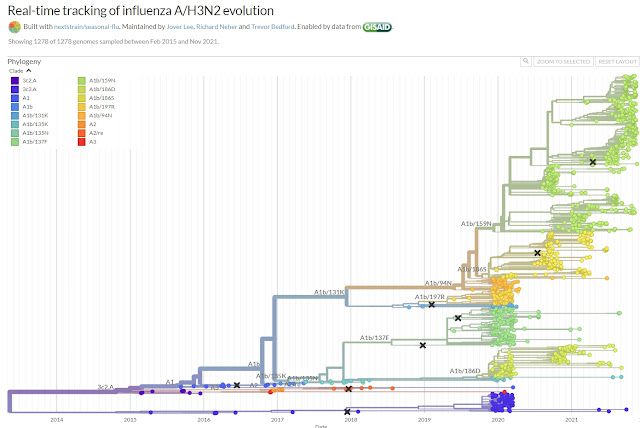 |
| Figure 6: The influenza A/H3N2 family tree (phylogenetic tree) shows all the genetic branches of H3N2 that have evolved since 2015. (Source: nextstrain) |
With fast-mutating viruses like influenza or coronaviruses, immune escape happens relatively quickly. With Omicron, some people with natural immunity (most likely those who were the first to catch the initial Wuhan strain) appear to be crossing the threshold of immune escape despite having long-lasting immunity to an earlier variant, as demonstrated by the aforementioned 141 studies showing a long-lasting adaptive immune response after infection. So, because of the rapid evolution of the virus, long-lasting immunity and immune escape are not contradictions after at all.
If Immune Escape is Inevitable, How Do We Create Long-Lasting Protection Against a Contagious and Rapidly Evolving Virus?
Frequent re-exposure solves the problem of a rapidly evolving virus by updating our immune system to recognize and neutralize closely related variants before we lose all our protective immunity from a previous infection. As long as the interval between exposures is not too long, you will still have cross-reactive immunity from your last exposure to protect you during your next "update". Re-infection does not necessarily mean you will get sick. As long as it happens while you still have partial cross-reactive immunity, your "update" might be mild, or you may not get any symptoms at all.
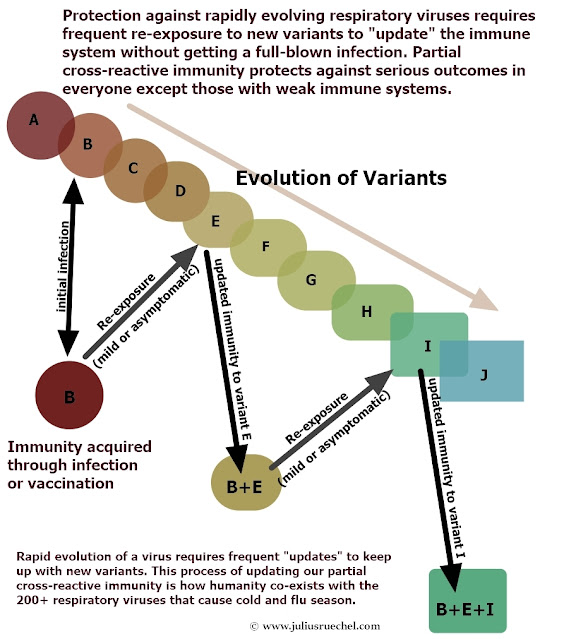 |
| Figure 7: To maintain immunity to a respiratory virus, your immune system needs periodic updates. But as long as you are re-exposed frequently enough, most re-infections will be mild or asymptomatic. |
In other words, we have to stop thinking of our immune systems as mere protective shields. They are much more than that. We need to remind ourselves that our immune systems are self-improving protective shields that need frequent exercise in order to maintain and update their skillset to keep up with an evolving enemy. The propaganda during Covid has not denied this fact, it has merely distorted it to the point where many people have lost faith in their immune systems, have become terrified about every "variant of concern", and have become fixated on vaccines as the only path to salvation. Fear doesn't just blind us to what is standing before our eyes. It also makes us doubt our own senses and forget our long-established understanding of the world.
Frequent re-exposure is nature's solution to booster shots. Vaccine boosters make more sense for diseases in which re-exposure is so rare that immunity wears off entirely before you are likely to get a natural update (more on that later).
It's worth reminding ourselves that there are over 200 respiratory viruses that cause colds and flus and yet, despite the fact that they are permanently circulating in our communities, we do not get sick with dozens and dozens of colds and flus every year. Although we won't be exposed to every single one of these 200 viruses every single year, we will cross paths with many of them. But as long as our immune systems have not been weakened by some serious pre-existing health condition (i.e. obesity, cancer, HIV, etc.) or by lifestyle choices that temporarily suppress our immune systems (i.e. poor sleep, lack of exercise, vitamin C or D deficiencies, stress, depression, isolation, etc.), most of these "updates" will merely be mild or asymptomatic infections because our immune systems encounter them so often. For every update that requires a Nyquil, your immune system probably has asymptomatic updates to dozens more every year without you ever noticing.
| Figure 8: A brief reminder that asymptomatic colds are nothing new. |
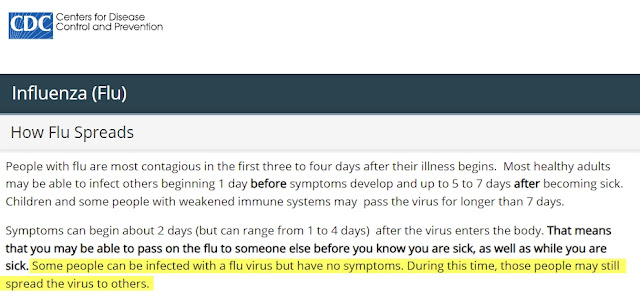 |
| Figure 9: A brief reminder that asymptomatic flus are nothing new either. |
There will always be some strains that are so unfamiliar to our immune systems that they cause a full-blown cold or flu. And there will always be some people whose immune systems are temporarily or chronically weak and are therefore at a higher risk of a serious outcome. But for most people, once we've been exposed for the first time, partial cross-reactive immunity protects us against severe outcomes during these periodic immunity "updates". For those who have already been infected by a previous variant of Covid during the last year and a half, Omicron is unlikely to ever be more than a mild or asymptomatic "update".
But what about our first contact with the dreaded Covid virus? By late February of 2020 it was already clear from epidemiology data from Italy and from the outbreak on the Diamond Princess cruise ship that even the very first infection with the SARS-CoV-2 virus poses very little risk to the overwhelming majority of people. By now we know why. Between 90 and 99% of the population already had partial cross-reactive immunity to SARS-CoV-2 thanks to previous exposure to other coronaviruses.
For most people, this virus was no more remarkable and no more dangerous than any of the other viruses that cause colds and flus every year. Yet during Covid, the media and public health officials have gone out of their way to de-emphasize the high number of people whose PCR-positive cases are completely asymptomatic (at least 40% of Covid cases are asymptomatic, and that was before mild Omicron came along!) Partial cross-reactive immunity is the unsung hero of the Covid crisis. It is the single most important virology concept of this pandemic, and it simply isn't being talked about in the News. But look... 👉👉👉vaccines!
The Importance of Frequent Exposure: Lessons from Malaria and the RSV virus.
A great example which illustrates the immune system training that occurs through frequent "updates" (and, more importantly, an example of the unfortunate consequences to our immune systems if we stop updating) comes from one of the deadliest diseases in the world: malaria. People who live in places where malaria is endemic (like around Lake Victoria in Africa) will catch malaria frequently. Children have the highest risk of dying because their immune systems have not yet had a chance to build up any background immunity. The first time is the most dangerous. But after a few infections the risk of dying from malaria is gradually reduced as a certain background immunity builds up.
Building immunity against the protozoa that cause malaria is much harder than building immunity against common respiratory viruses like coronaviruses or influenza. It takes around 20 years of frequent exposure to malaria to train the immune system to develop a certain background immunity (it's a very complicated disease!). Background immunity to malaria never prevents infection - my Kenyan wife speaks of catching malaria many times during her childhood, each bout as hellish as the last - nor does it fully eliminate the risk of death. A safe malaria vaccine would be a Godsend if it could be developed. But previous infections with malaria do nevertheless reduce the risk of death during subsequent re-infections.
But if people who have built up this background immunity move someplace where there is no malaria, their background immunity begins to fade. Use it or lose it. As our travel medicine clinic explained to my wife, if she is exposed now, many decades since her last bout with the disease, she has been away from Kenya for so long that she can no longer count on having any background immunity to malaria. Research has shown that it fades within 3 to 5 years without re-exposure.
This concept of losing a previously acquired background level of immunity is called an immunity debt. Through a lack of repeat exposure, my wife's background immunity to malaria has waned and she may now be nearly as vulnerable to a severe outcome as someone like me who did not grow up around malaria and has never been infected. For many diseases, frequent re-exposure is essential to maintain protective immunity.
This also applies to the 200+ rapidly evolving respiratory viruses that cause our colds and flus every winter. And it also applies to Covid. Use it or lose it.
If we interrupt regular exposure to any of these common respiratory viruses, such as through lockdowns and extreme social distancing measures, we prevent ourselves from getting the regular exposure needed to keep training our immune systems to keep them up to date. The key to living a healthy life is to never stop living a normal life.
An immunity debt to our common respiratory viruses can happen after a surprisingly brief period without regular exposure. The immunity debt caused by a year and a half of lockdowns and school closures is already causing cases of RSV virus (another common respiratory virus) to surge to unprecedented levels among children. Prior to the Covid debacle, most RSV infections were relatively mild, with symptoms similar to a common cold (prior to 2021 you'd probably never even heard of this virus unless you work in the medical profession). But now, with an immunity debt, far more cases are becoming dangerous. New Zealand hospitals were recently flooded with children hospitalized by the RSV virus. Children's hospitals in Canada reported the same recent surge in RSV cases caused by this immunity debt.
 |
| Figure 10: November 9th, 2021, article in CBC News: CHEO sees record number of patients with non-COVID respiratory virus |
Here's the most important excerpt from the CBC article:
 |
| Figure 11: Excerpt from the November 9th, 2021, article in CBC News: CHEO sees record number of patients with non-COVID respiratory virus |
Dr. Pascal Lavoie, a pediatrician and clinician scientist at the B.C. Children's Hospital Research Institute in Vancouver, was quoted in the linked CBC article as follows: "Our immunity against some viruses has gone down simply because, for some viruses, our protection depends on being repeatedly exposed."
An ER doctor in Nova Scotia reported recently that up to 20% of the patients coming to the ER in her hospital have RSV! It seems we are now paying the piper for the immunity debt created by the lockdowns and social distancing measures recklessly imposed on society by our public health officials and politicians.
 |
| Figure 12: December 4th, 2021, article in CBC News: ER doctor concerned by rise in dangerous respiratory virus in N.S. children |
Experts are also warning of a particularly bad flu season this winter because this immunity debt also extends to all the other viruses that cause colds and flus. Thanks to the immunity debt caused by our out-of-touch governments, suddenly all these other 200+ respiratory viruses are seeping into public consciousness. But never let a good crisis go to waste. Now the public can be boondoggled into accepting vaccines for those too.
Would it surprise you to learn that Moderna has now begun working on a vaccine against the RSV virus, which could be combined with the Covid vaccine as a single jab? And that the hunt has begun for a "super-vaccine" that can stop not just the Omicron variant, but all the other four coronaviruses that cause 15-30% of colds and flus every winter? And that a combo Covid-influenza vaccine is also already in the works? This is government-corporate corruption at its finest — create the problem and then sell you the cure. As the saying goes, "don't ever let the government help you because once they get involved, you'll never get rid of 'em."
On so many levels, the current misbegotten public health policies are increasing the risks they are claiming to try to prevent. We are being held hostage by the most destructive, counter-productive, and predatory public health experiment in human history.
Even if the Covid vaccines worked as advertised (they don't: more on that in a moment) and even if they didn't cause dangerous adverse reactions in many people (they do: more than 19,000 deaths and 1.7 million injuries have been reported to date just on the US VAERS system alone), these Covid vaccine boosters are merely artificial replacements that are trying to replicate what the immune systems of healthy people are naturally evolved to do by themselves through repeat exposure. Our public health officials and vaccine makers are making mountains out of molehills while creating entirely unnecessary new vulnerabilities in order to sell you something that most people do not need if they are allowed to live normal lives.
 |
| 2021: the year that humans were transformed into pincushions (image by Dvortygirl, CC BY-SA 3.0) |
If We Get Natural "Updates" Through Re-Exposure, Why Do We Give Booster Shots for Many Other Diseases That Are Included in Childhood Vaccination Programs?
Ah, you might say, then why are periodic booster shots recommended as the go-to strategy to protect us against many other diseases? Why don't we also simply rely on frequent natural exposure to diseases like tetanus, rubella, pertussis, and shingles to protect us after our initial immunizations to those diseases?
As I explained in my article, The Snake-Oil Salesmen and the COVID-Zero Con: A Classic Bait-And-Switch for a Lifetime of Booster Shots (Immunity as a Service), the natural immunity we acquire from infections with the rapidly evolving respiratory viruses that cause our common colds and flus only tends to protect us for a few months to a few short years before we become vulnerable to re-infection. Consequently, almost everyone will re-catch (and spread) some of these respiratory viruses every single year. So, unless you live on a deserted island, you cannot go many years without re-exposure. You will get semi-regular "updates" just by living a normal life.
But let's compare that to something like chickenpox. Immunity to chickenpox lasts at least 10 to 20 years. This means that, in any given year, the maximum number of people who can get infected and who can spread chickenpox to others is very very low. Consequently, it is very easy to spend decades of our lives without ever being re-exposed even after our immunity has faded away. Prior to the start of chickenpox vaccination programs in the USA, there were only about 4 million cases per year in the USA... in a country of over 250 million (in 1990). Long delays between exposure mean that by the time our immune systems are finally re-exposed, our immunity may be so out of date that we can get the full-blown disease rather than just a mild update.
Since chickenpox vaccination was introduced in the 1990s, symptomatic cases in the community have fallen even lower (even as the population has grown to over 330 million). With vaccination reducing the number of children coming home from school with symptomatic chickenpox, it is now even less likely that people will be exposed to chickenpox at sufficiently frequent intervals to update their immune systems without putting themselves at risk of severe consequences.
Compounding this is the fact that most respiratory viruses cause relatively mild re-infections (except among those who have compromised or weak immune systems). By contrast, a re-infection with many of these other diseases poses a severe risk even to those who have strong immune systems. A re-infection as an adult with the varicella-zoster virus (the virus that causes chickenpox) often leads to the Shingles version of the disease which, while rarely life-threatening, can lead to serious life-long debilitating problems like blindness.
So, the lack of opportunities for frequent re-exposure and the dangerous nature of these other diseases mean that boosters are a much lower-risk strategy for updating our immunity to them.
However, as a brief aside, it must be said that the conflicts of interest, lack of transparency, lack of debate, relentless propaganda, and the reckless disregard for safety and human rights displayed by our public health institutions, all of which have been exposed in stark contrast during the Covid debacle, means that these institutions urgently need to be reformed in order to restore integrity to the certification and safety monitoring processes for vaccines and other pharmaceutical drugs. These rotting institutions have no-one to blame but themselves for the collapse of trust in their services; they have a long road ahead of them to earn back public trust in their role as objective and responsible stewards of public health. We all have a lot to lose if these institutions are allowed to continue on the path they are on.
The Dirty Trick Played With "Variants"
SARS-CoV-2 is here to stay. It is endemic. That has been clear since February of 2020 to anyone that understood the implications of Covid's high infection rates and the high percentage of infections that produce mild or asymptomatic cases. The genie could never be caught and put back in the bottle. Many of our public health officials are finally beginning to admit this obvious fact even as they continue to stoke fear about variants. Here is Dr. Bonnie Henry, Provincial Health Officer of British Columbia, admitting that SARS-CoV-2 is endemic.
Rochelle Wallensky, the director of the US CDC, has also admitted it is endemic. The WHO has even announced it will name future variants after star constellations once they run out of letters in the Greek alphabet, which is an acknowledgement that they know this virus is here to stay, joining the other 200+ endemic viruses that cause colds and flus every year. Variants are normal.
The only unusual thing about Covid is the rather bizarre obsession with naming and tracking variants on the 6'oclock news despite the fact that we don't do this for any of the other 200+ viruses that cause cold- and flu-like symptoms every year. But since our public health officials and media are making a fuss about variants and threatening us with more boosters, let's have a closer look at the big picture and not just at the elephant's tail that they're waving in our faces.
The chart below shows how much the genetics of the SARS-CoV-2 virus have changed since it emerged in 2020. Dark blue is the Alpha variant. Light blue is the Delta variant. Omicron is showing up in red. It will never stop evolving and producing new variants.
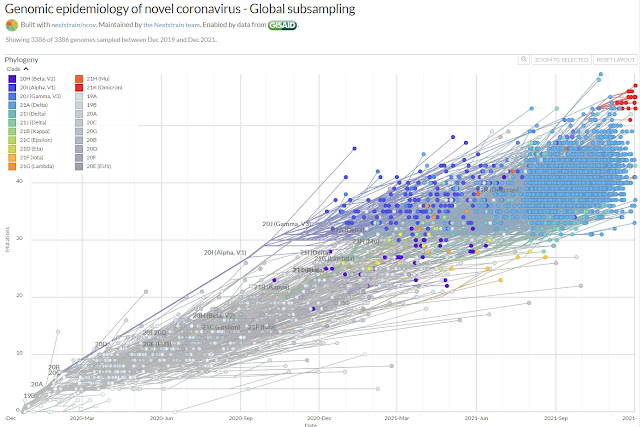 |
| Figure 13: Evolution of the SARS-CoV-2 virus over time, showing how much its genetics have changed since the Wuhan strain first emerged at the beginning of 2020. (Source: nextstrain) |
And this chart of the SARS-CoV-2 family tree shows all the variants that have evolved over time. The Delta variant, which was dominant worldwide until recently, is in light blue while the new Omicron variant is shown in dark red.
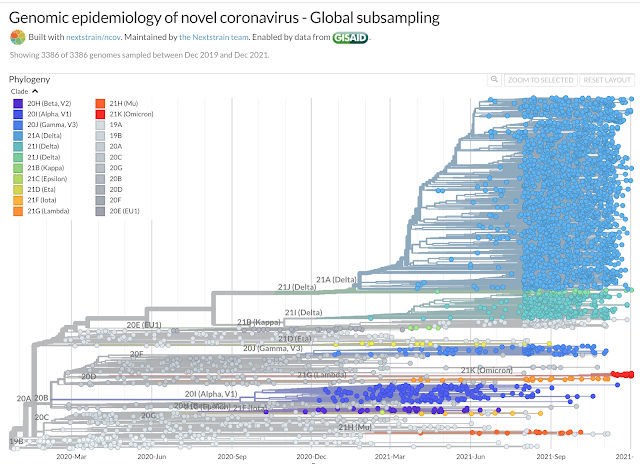 |
| Figure 14: The SARS-CoV-2 family tree (phylogenetic tree) showing the emergence of Covid variants over time. (Source: nextstrain) |
As you can see, the virus is not a linear evolution of one mutation following on the heels of another. In reality, each variant is more like a swarm of closely related particles, but none of those particles are carbon copies of one another, and most branches and sub-branches in the family tree will become evolutionary dead ends. From time to time, the swarm from one variant crowds out a swarm from another variant, just like the original Wuhan strain was crowded out by Alpha, which was crowded out by Delta, which is now in competition with Omicron.
Each "variant" swarm essentially acts as an entirely new and separate albeit closely related pandemic, which follows on the heels of the previous one. The original virus (Wuhan-strain) and the Alpha-strain are gone, never to be seen again. They are as extinct as the woolly mammoth. Your immunity to these extinct variants can only ever benefit you by providing cross-reactive immunity to closely related future variants because your immune system will never see either of these two variants again. Only their descendants and their closely related cousins remain. The Delta strain. The Mu variant. The Lambda variant. Omicron.
If this was about public health, they would only be offering vaccines to the vulnerable, without coercion. But the Holy Grail of maximizing pharmaceutical profits and public health funding was to convince the public (and politicians) that there is something unusual or threatening about the never-ending conveyor belt of variants produced by a rapidly evolving and highly transmissible virus, and (as Pfizer's CEO suggested at the beginning of this article) that relying on natural immunity could lead to more variants. It is a masterful manipulation held together by endless half-truths.
Influenza and coronavirus were the two perfect candidates for this kind of never-ending universal vaccination boondoggle since they produce lots of "variants" and since immunity to these rapidly evolving viruses will never last long (because natural immunity to these viruses fades quickly and because rapid genetic drift quickly leads to immune escape without regular re-exposure).
The Holy Grail comes into reach if the public can be bamboozled into thinking that they are left unprotected and therefore require constant boosters to keep up with variants. By naming each variant, using widespread PCR tests on mild and asymptomatic people, and endlessly streaming out-of-context case numbers, hospitalizations, and deaths on the television, they have terrified society to the point where many people absolutely do not want to be exposed to any of these variants, ever, at any cost. And so, vaccine boosters provide a technological escape from the scary shadow that Big Pharma and public health have projected up onto the wall. Keep the public scared and they will just keep running back for more boosters, for as long as the panic can be kept intact or until politicians can be convinced to make boosters mandatory with criminal consequences for those that refuse them.
Prior to July of 2008, the WHO defined an influenza pandemic as: "An influenza pandemic occurs when a new influenza virus appears against which the human population has no immunity, resulting in several, simultaneous epidemics worldwide with enormous numbers of deaths and illness... " But in July 2008 they revised the definition to eliminate "with enormous numbers of deaths and illness," thereby giving themselves the option to declare a pandemic whenever there is a rapidly spreading variant of any virus, regardless of how deadly it is. That's how we got to the 2009 Swine Flu vaccination debacle and now to Covid.
Removing the "enormous numbers of deaths and illnesses" clause from the definition of pandemic was the chess move that opened the door to permanent crisis. It's no longer deaths that provide an objective measure of risk, only positive PCR tests, which are being forced en mass on the entire population, despite high false positive rates and despite the fact that most people who are forced to take these tests are not grievously ill and may never experience anything more than a mild or asymptomatic infection. A virus with a scary and unfamiliar name producing a never-ending supply of new "variants of concern" provides the perfect cover to maintain a never-ending panic about never-ending waves of pandemics requiring never-ending booster shots "to keep us safe". A whopper of a big lie built on a vast architecture of half truths.
And in case anyone asks why the world has suddenly been engulfed by a never-ending series of pandemics, there's a ready excuse for that too. From USA Today: "Scientists are seeing an 'acceleration of pandemics': They are looking at climate change."🙄 How convenient.
But let's get back to reality. The chart below from the UK shows what these successive variant "pandemics" look like as they compete with one another for hosts until one manages to outcompete the others and become dominant, only to be replaced a short time later by another more competitive variant. Most of the time, the most contagious but least dangerous variant wins the race because spread is maximized if a variant can infect as many people as possible without confining them to bedrest (a person confined to bedrest doesn't mingle with as many people as a person fit enough to go to the pub). That's why, as a rule of thumb, most viruses tend to evolve towards being more contagious but less dangerous over time. Focusing on cases (which increase as a virus becomes less dangerous) allows public health officials to keep the panic going even as the virus loses its ability to cause as many deaths. Look, cases... 👉👉👉we need vaccines!
In the UK, the EU1 variant (beige) squeezed out the original Wuhan strain (grey) in late summer of 2020. The Alpha variant (red) squeezed out the EU1 variant during the winter of 2020/21, and the Delta variant (green) replaced the Alpha variant during the summer of 2021.
 |
| Figure 15: In the UK, Delta achieved dominance earlier than in the USA. Source: https://covariants.org/per-country. |
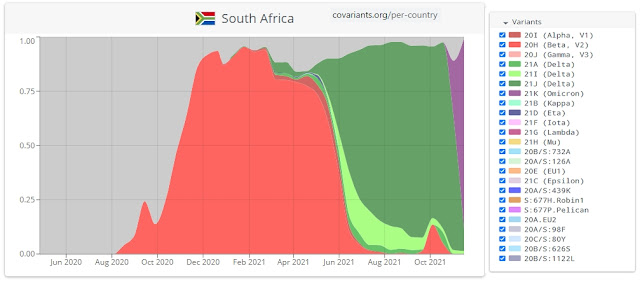 |
| Figure 16: In South Africa, the Omicron variant only appeared very recently, but has already almost completely displaced Delta. Source: https://covariants.org/per-country. |
As you would expect as a virus evolves towards becoming less dangerous, despite surging Omicron infections (confirmed by PCR testing), doctors from South Africa are reporting that hospitalizations are NOT surging despite the fact that to date only 25% of its population has had 2 jabs. And among the small number of Covid-positive hospitalizations in South Africa, a full 76% of those Covid-positive patients were actually hospitalized for reasons completely unrelated to Covid. The lack of hospitalizations caused by Omicron shouldn't surprise anyone. Based on antibody testing, by August of 2021 approximately 80% of South Africa had already been infected by the SARS-CoV-2 virus. For most South Africans, Omicron is merely an update.
All the fuss about Omicron is like freaking out about a giant ball of fire that will rise on the Eastern horizon tomorrow morning to bombard our planet's fragile atmosphere with a flood of photons and ultraviolet radiation, also known as the Sun for those who can see the full elephant. It's high time that life was allowed to go back to normal.
The 141 studies noted at the beginning of this article demonstrate that natural immunity lasts more than long enough to get us through the next few seasonal waves of Covid armed with plenty of partial cross-reactive immunity. Breakthrough infections are happening with Omicron. But people aren't keeling over in droves, demonstrating that partial cross-reactive immunity is working as it should. Our natural immunity will be updated with very little risk of ending up with any kind of grave illness. Just like what happens every year with the other 200+ viruses that cause colds and flus, largely without ill effect for most of us, despite having to take great precautions to protect our most vulnerable and elderly.
By contrast, the immunity offered by vaccination is proving far less suited to the task of updates...
The Bitter Pill: How Long Does Immunity Last After Vaccination?
I have written at length in previous articles about the high and rising number of serious and deadly adverse reactions to the Covid vaccines, the lack of long-term safety data, the dangers associated with using a leaky vaccine for mass vaccination, the absurdity of vaccinating those who have recovered from the disease, the inappropriateness of offering vaccines to those who have little to no personal risk to offset, and the fact that making them mandatory is a violation of bodily autonomy. The most important of those deep dives are found in my recent book, Autopsy of a Pandemic #CommissionsEarned, so I won't rehash any of that here.
Nor will I dwell on the obvious fact that you cannot protect the vulnerable by vaccinating everyone else with a "leaky" vaccine that does not stop the vaccinated from getting infected and that does not stop the vaccinated from spreading the virus to others. The vaccinated are not just equally at risk of being infected as the unvaccinated, official data from the United Kingdom even shows that infection rates among the vaccinated exceed infection rates among the unvaccinated. Some vaccine. It has become a pandemic of the vaccinated. Oops.
 |
| Figure 17: In the UK, infection rates among the vaccinated exceed infection rates among the unvaccinated in all age groups above the age of 18. (Source: UK Health Security Agency's Week 41 Covid-19 Vaccine Surveillance Report, published October 14th, 2021) |
Research studies have even conclusively demonstrated that there are no significant differences in viral loads between vaccinated and unvaccinated individuals who catch the virus. In other words, there is no difference to how contagious a vaccinated person is compared to an unvaccinated person. Barring the unvaccinated from normal life doesn't reduce anyone's risk whatsoever. As a technology, these vaccines are a seriously flawed piece of kit.
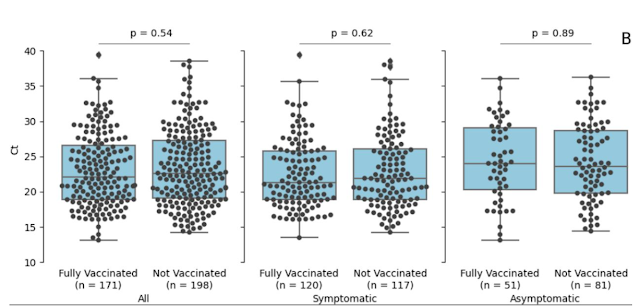 |
| Figure 18: There is no significant difference in viral load between vaccinated and unvaccinated individuals (Acharya et al) |
But aside from all those other disqualifying catastrophes, how much individual protection do the vaccines provide to those who have rolled up their sleeve for the magic elixir? Even in this regard, the vaccines were failing miserably as a tool to provide meaningful "updates" against the SARS-CoV-2 virus (and that was before the vaccines became obsolete in countries where the vaccine-resistant Omicron variant now dominates (i.e. South Africa, South Korea, Netherlands, Finland, Ghana, Thailand, Hong Kong, and the list grows by the day - you can watch Omicron take over, country by country, on the CoVariants website):
Like all seasonal respiratory viruses, infections with the SARS-CoV-2 virus come in waves that are strongly seasonal in nature. In the northern hemisphere, we are at the start of the current winter flu season. If you are infected between now and the Spring of 2022, you probably won't be re-exposed to the virus again until the next big seasonal wave during the winter of 2022/23, 9 to 12 months later. Consequently, immunity gained from an update needs to last a minimum of 12 months to provide any meaningful cross-reactive immunity to future variants. 24 to 36 months would be better because, like all colds and flus, we are unlikely to all be exposed to every single season's new variant - we might miss a year or two between exposures.
Vaccine makers and public health institutions hit the public funding jackpot when they convinced politicians of the necessity to mandate boosters for everyone to replace the natural updates that occur after reinfection. At first, they seemed to steer towards a 12-month booster — an artificial annual replacement for what your immune system is capable of doing on its own through frequent re-exposure.
But then they revised their booster program down to 6 months. Now it's been revised again so that boosters are going to be offered to all adults after just 3 months. Here's a link to a clip of the UK's Health and Social Care Secretary, Sajid Javid, making the case to reduce the minimum dose interval from 6 months to 3 months and stating that the booster program should be expanded beyond the vulnerable to include all age groups over the age of 18.
Why the sudden acceleration?
The vaccines are failing even before Omicron. The following chart from a paper published by the Lancet (preprint) shows how quickly the protection from the vaccines fades as a strategy to prevent symptomatic infections.
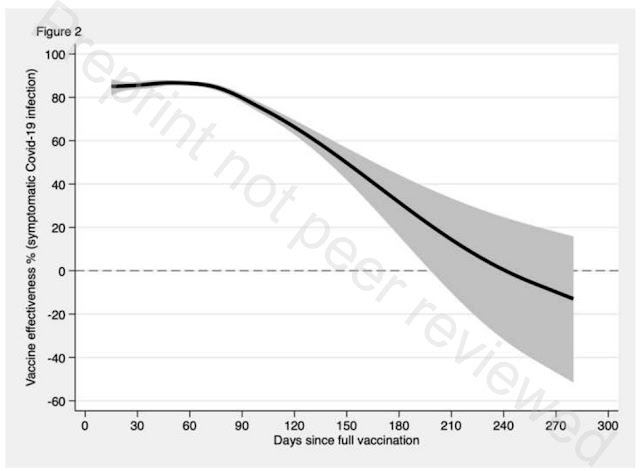 |
| Figure 19: Covid vaccine effectiveness to prevent symptomatic infection (source: The Lancet preprint - you have to download the full-length pdf linked at the bottom of the abstract and scroll to the bottom to find the graphs.) |
The first 90 days holds relatively steady, but then things fall apart. After 90 days, protection begins to fall off rapidly. By 6 months, it is nearing zero. By 9 months it has fallen below zero. Negative protection. Say what?
Negative protection means that people become more susceptible to a Covid infection than if they had not been vaccinated at all. What began as protection slowly dwindles away and actually becomes a vulnerability.
The same study also shows how effective the vaccine is in stopping severe outcomes (i.e. hospitalizations and deaths). Again, the first 3 months look rosy and then it all fades away, with the lower portion of the error bands falling below zero by 6 months:
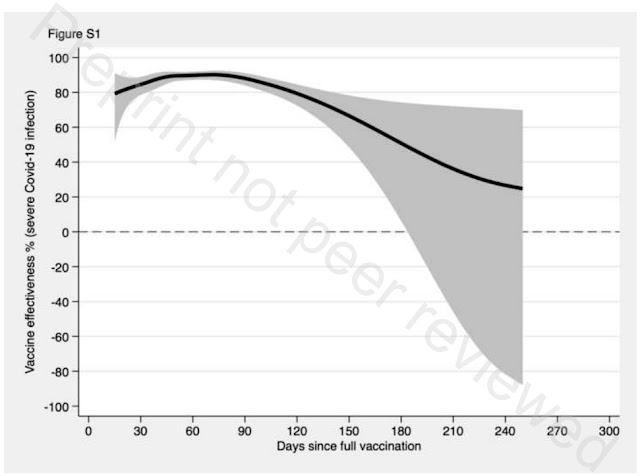 |
| Figure 20: Covid vaccine effectiveness to prevent severe infections (source: The Lancet preprint -you have to download the full-length pdf linked at the bottom of the abstract and scroll to the bottom to find the graphs.) |
The fact that protection turns negative after the initial protection wears off suggests that the worse-case warnings offered by the likes of Dr. Sucharit Bhakdi and Dr. Geert Vanden Bosche are coming true. The vaccines appear to be triggering some kind of antibody-dependent enhancement as protection fades, which makes it easier for the virus to infect vaccinated people (and more likely that they have a severe infection) once their vaccine-induced immunity begins to wear off. The unanswered question is whether that negative immunity is temporary and whether the effect gets worse or better as you keep filling up your Pfizer loyalty card:
Don’t forget to get your #pfizer loyalty card after 7 boosters and a get a free toaster 😂 #Booster pic.twitter.com/fVV2ZMzACk
— Jonathan Toop (@JonT4) December 1, 2021
And then there's the little problem raised by the study published in medRxiv (preprint) on December 8th, mentioned at the start of the article, which demonstrates that the current batch of vaccines are no longer properly neutralizing the Omicron variant even from day one of vaccination. Oops.
Things fall apart. The more the vaccines fail, the more our public health officials and vaccine makers double down. They have little choice now. The Quest for the Holy Grail of Pharma-utopia has trapped them too. If the scam falls apart, people will start asking questions and calling for their heads. So, in under a year they have gone from voluntary vaccines for the vulnerable, to coerced mass vaccination of all age groups, to forcing compulsory vaccination on unwilling citizens (with fines and jail time now being rolled out against citizens in Austria and Germany who refuse - more details about Austria's grotesque mandatory vaccination law here), and there are now efforts underway to make the vaccines compulsory in all of the EU. Even Dr. Fauci seems to be trying to warm the US up to the idea of compulsory vaccination. The desperation is becoming palpable:
Fauci: "I would prefer, and we all would prefer that people would be voluntarily getting vaccinated, but if they're not gonna do that, sometimes you've got to do things that are unpopular, but that clearly supersede individual choices..." pic.twitter.com/yxbOw9cwKw
— The Post Millennial (@TPostMillennial) December 8, 2021
Variant by variant, they are trying to turn us into dependent pincushions. Knowledge gives us immunity to their propaganda. Stopping the madness is a numbers game, so never give up trying to help friends and family see the full elephant that our public health institutions, media, and vaccine makers are trying so hard to prevent them from seeing. Please share this article widely. When enough of us say "No", enforcement of this medical tyranny becomes impossible.
~
IT was six men of Indostan
To learning much inclined,
Who went to see the Elephant
(Though all of them were blind),
That each by observation
Might satisfy his mind.
II.
The First approached the Elephant,
And happening to fall
Against his broad and sturdy side,
At once began to bawl:
"God bless me!—but the Elephant
Is very like a wall!"
III.
The Second, feeling of the tusk,
Cried: "Ho!—what have we here
So very round and smooth and sharp?
To me 'tis mighty clear
This wonder of an Elephant
Is very like a spear!"
IV.
The Third approached the animal,
And happening to take
The squirming trunk within his hands,
Thus boldly up and spake:
"I see," quoth he, "the Elephant
Is very like a snake!"
V.
The Fourth reached out his eager hand,
And felt about the knee.
"What most this wondrous beast is like
Is mighty plain," quoth he;
"'Tis clear enough the Elephant
Is very like a tree!"
VI.
The Fifth, who chanced to touch the ear,
Said: "E'en the blindest man
Can tell what this resembles most;
Deny the fact who can,
This marvel of an Elephant
Is very like a fan!"
VII.
The Sixth no sooner had begun
About the beast to grope,
Than, seizing on the swinging tail
That fell within his scope,
"I see," quoth he, "the Elephant
Is very like a rope!"
VIII.
And so these men of Indostan
Disputed loud and long,
Each in his own opinion
Exceeding stiff and strong,
Though each was partly in the right,
And all were in the wrong!
MORAL.
So, oft in theologic wars
The disputants, I ween,
Rail on in utter ignorance
Of what each other mean,
And prate about an Elephant
Not one of them has seen!


Comments
Post a Comment