Cancer Rates are Increasing -- and May Get Much Worse
Cancer Rates are Increasing -- and May Get Much Worse
Wiped Out Immune Systems Take Time to Manifest
We have a problem: cancer deaths began to increase, off the charts, in late 2021, with cancer death incidence exceeding expected levels by a statistically “impossible” 9-sigma difference — and we are seeing only the first small ripple of a storm coming in the future.
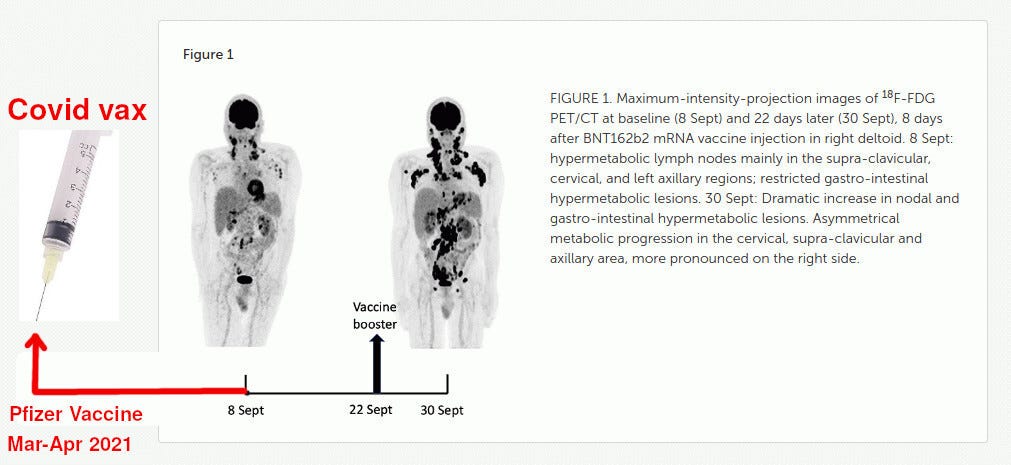
Nobody exemplifies this wave of cancers better than the Belgian Covid vaccine advocate and misinformation fighter Michel Goldman, who developed a “rare” form of lymphoma (immune system cancer) following his Covid vaccination. His lymphoma rapidly worsened after his booster dose and Michel’s chance of 5-year survival is below 30 percent.

Michel Goldman is not an ordinary citizen. He is a lifelong promoter of vaccines and a famous immunologist. For example, Prof. Goldman lamented the slow vaccine rollout in the EU in a high-profile article from April 2021. He expressed dismay over pausing the AstraZeneca vaccine due to a “very small” number of thrombosis cases, as the pause could “fuel distrust in all Covid vaccines”, and admonished EU leaders that they must “must urgently accelerate the region’s COVID-19 vaccine rollout”.

Ironically, the above article was written on April 2, 2021, almost exactly when Michel was getting his second dose of the Pfizer vaccine - that caused his cancer.
Prof. Goldman is also cited in fact-checks such as this one:

The fact check (which did not age well in general, unlike Dr. Malone’s article) says:
For instance, human trials for a cancer mRNA vaccine have been going on since at least 2011. As Michel Goldman, a professor of immunology at the Université Libre de Bruxelles, explained: “If there was a real problem with the technology, we’d have seen it before now for sure”.
What is odd is that at the time the above fact check was written in Dec 2021, Michel Goldman already knew that Covid vaccine and booster caused his lymphoma and that he was fully aware that he already was in Stage IV of the disease.
So you can see that this vaccine-caused lymphoma could not have happened to a nicer guy!
The Atlantic Article, as well as the scientific article authored by Michel Goldman himself, describing his own cancer, glosses over the fact that his cancer was not just accelerated, but was initiated by the Pfizer vaccine. Here’s the picture from Michel’s scientific article, edited by me for clarity (my addition is in red). It shows that Prof. Goldman received the initial dose of the Pfizer Covid vaccine six months before his cancer diagnosis:
While I wish Prof. Goldman a speedy recovery from his advanced cancer, he is not alone.
Unprecedented 9-Sigma Increase Increase in Cancer Deaths in the US
There are thousands of “Michel Goldmans” in just the United States, most of whom are not as famous, but more unlucky compared to Michel. Unlike Michel, who is still alive, those thousands of people in the death statistics are already dead — and they possibly would not die if not for the Covid vaccines.
The Ethical Skeptic on Twitter has been analyzing US mortality (which is reported by the CDC on a weekly basis), which is a very difficult job due to the CDC’s strange, never-ending “system upgrade” that magically seems to hold back a lot of deaths and reclassified cancer deaths into Covid deaths.


He discovered the misclassification and corrected it, to show the true number of cancer deaths:

The lighter line is the actual number of cancer deaths, and the darker line is the expected number — showing a never-seen-before increase in cancer deaths that is deepening. As of several recent weeks, the United States has about 800 excess cancer deaths per week. As you can see on the right side of the graph, these excess deaths started just as Covid vaccination took off, and never slowed down or returned to normal; they are increasing and showing acceleration.
Similar Increases in the UK
The UK had 10-17% excess all-cause mortality in the last few months, and the concerned British government put up an “Excess Mortality Presentation”, showing
us these excess deaths in a variety of ways. The page for cancer deaths is here:
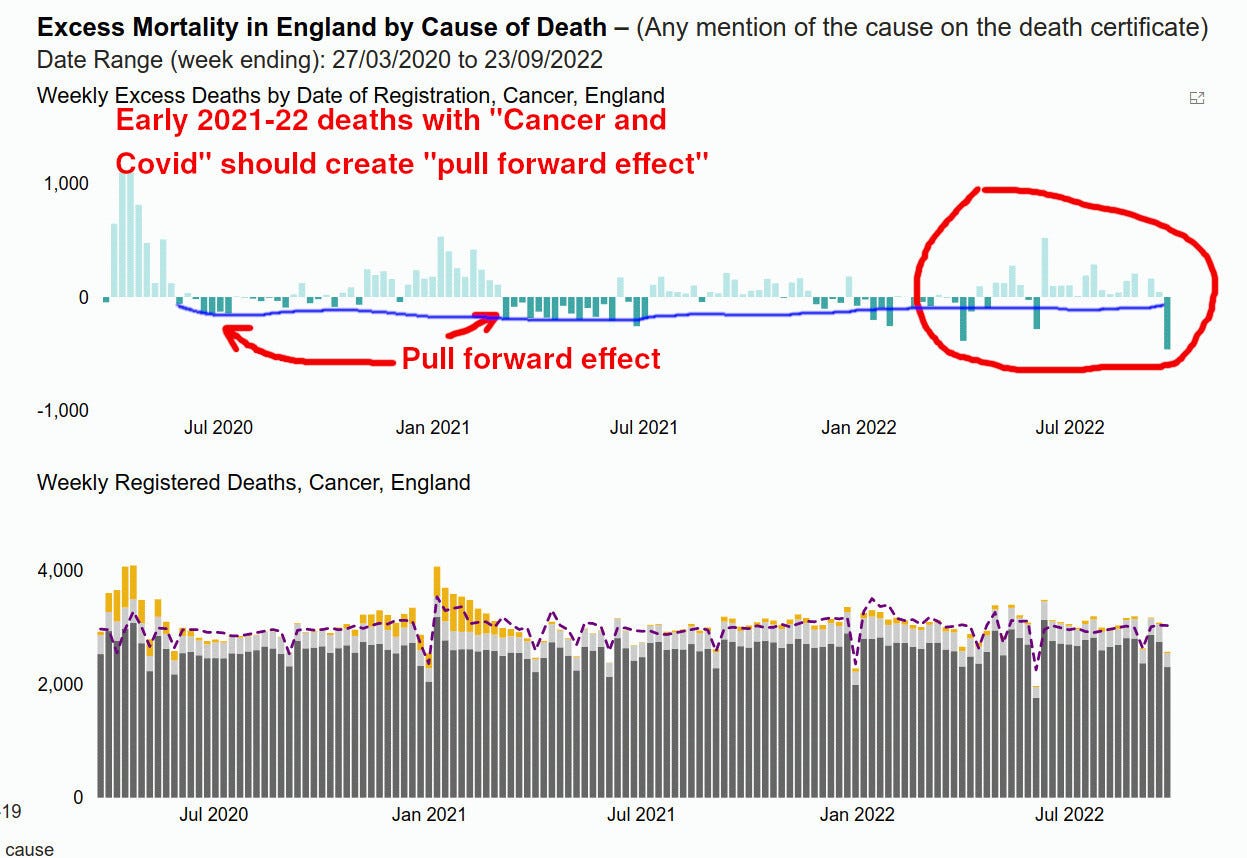
Pull-Forward Effect
Unlike the Ethical Skeptic data, the UK presentation is NOT adjusted for the “pull-forward effect”, that is, the fact that many cancer patients already prematurely died with Covid in 2020-early 2021. Had the Covid pandemic not happened, these patients would be dying somewhat later, such as in 2021 or 2022.
Therefore, had no additional “factor” introduced excess cancer mortality in 2021, these early deaths with “Covid and cancer” would have resulted in a lowered rate of cancer deaths in 2021 and 2022 — so the excess deaths shown in the above presentation UNDERSTATE the true extent of excess deaths.
I used a BLUE line on the above UK chart, to qualitatively show the pull-forward effect and how it underscores that the excess cancer deaths are somewhat understated.
Since the UK excess mortality data is available for download, I took a look at May-August excess cancer deaths, a total of 1,990 deaths.
For May-August of 2022, these excess cancer deaths amount to 110 excess cancer deaths per week. Had the UK’s population (68M) been the same as the United States (330M), that difference would amount to 550 excess cancer deaths per week, which is comparable to the Ethical Skeptic’s 800+ deaths a week. Again, The Ethical Skeptic’s numbers are adjusted for the pull-forward effect and the UK data is not so adjusted. The UK excess cancer mortality would be somewhat higher if adjusted comparably.
So, our calculations show that the UK and the US experience roughly similar excess cancer mortality. Anecdotally, we are seeing more rapidly developing cancers, that Etana Hechts calls “Turbo-cancers”.
Just to be clear: these increases do NOT show causation, just as Michel Goldman possibly was an extremely unlucky victim of a coincidence. (It was not a coincidence, as Brian Mowrey’s post and Goldman’s own article explain and refer to Goldman’s RHOA G17V mutation).
We do not yet have the smoking-gun level proof. We only have a suspicion, fueled by the temporal coincidences of this excess cancer mortality with the vaccination campaign. To know for sure, we need to compare outcomes in vaccinated persons versus unvaccinated persons — something that the UK and the US health authorities are not allowing.
These Excess Cancer Deaths are Likely a Sign of Much Bigger Future Increases
This part of the post is written by A Midwestern Doctor, whose substack I highly recommend. Midwestern Doctor explains why Covid vaccines are genotoxic, and mutagenic and have other effects to increase the rate of cancers far beyond what we have experienced.
Are Spike Protein Vaccines Genotoxic?
Before the mRNA vaccines entered the market, significant concerns existed regarding their cancer-causing potential. Despite this, as leaked documents from the EMA (Europe’s FDA) show, Pfizer (and most likely the other manufacturers) was exempted from testing their vaccines for genotoxicity before proceeding to human trials. To quote some of the leaked EMA documents:
“No genotoxicity has been provided. The components of the vaccine formulation are lipids and RNA that are not expected to have genotoxic potential. That being said, the novel lipids possess an acetamide moiety which is classified as possible human carcinogen (IARC Group 2B) with debated genotoxic mechanism, which should be discussed further…as the lipids contain an acetamide moiety which has been linked to carcinogenicity in animals, including liver tumors, potentially related to genotoxicity, and liver distribution and functional effects have been observed in rat, an extended discussion of these lipids is requested.”
As this testing was typically required for any new pharmaceutical and relatively easy to do, I interpreted it to mean that Pfizer had discovered their vaccine caused significant genotoxicity and felt their best option was to pretend they had never studied it so they would have plausible deniability when cancers inevitably emerged in the future (pharmaceutical companies frequently fail to report undesirable results as they almost never suffer consequences for doing so—the SSRI saga which in many ways is the best precedent we have for the current debacle is the only case I know of where pharmaceutical companies were eventually penalized by the courts for this criminally deceptive behavior).
As the vaccines began to enter the market, I then began noticing countless media outlets state that the vaccines could not change your DNA and that anyone who thought so lacked a basic understanding of science. When I looked at the evidence for this claim, I could not help but notice no direct evidence for it was provided, and rather the basis for the claim was an expert’s authority or three common logical arguments (e.g. consider these statements by Paul Offit and Anthony Fauci):
1. The vaccines cannot enter the nucleus of the cell
2. mRNA from the vaccines breaks down rapidly in the cell, so it does not have time to enter the nucleus and change your DNA.
3. mRNA is not DNA, and hence believing it can change DNA represents a fundamental lack of knowledge of biology.
The problems with these arguments were that:
1. The lipid nanoparticles can traverse the cell membrane, so it is entirely possible they can also traverse the nuclear membrane. Additionally, the highly positive charge of the spike proteins suggests they may be attracted to or able to bypass the negatively charged nuclear membrane [this was subsequently proven].
2. A major issue with the mRNA technology was that foreign mRNA is rapidly broken down by the body and therefore degrades before the desired proteins can be synthesized. To solve this problem, the manufacturers randomly added pseudouridine to the mRNA product, allowing it to resist degradation (and persist for at least 60 days).
Random pseudouridation was potentially problematic because:
•Persistent mRNA can produce an excessive dose of the spike protein product.
•Dysregulation of pseudouridation is associated with a variety of cancers.
•Pseudouridation is known to suppress innate immunity (which is necessary for a variety of things including eliminating cancers within the body).
3. RNA (including mRNA) can become DNA with the aid of retrotranscriptases. In addition to many viruses doing this, natural reverse transcriptases also exist within human cells.
I was thus less than surprised to learn researchers had discovered SARS-CoV-2 had done the impossible and had been observed to change the DNA of infected patients.
Not long after, when independent researchers finally examined the big question, they discovered that despite all the reassurances to the contrary, the mRNA vaccines did change liver cell DNA within 6 hours of exposure. In parallel, as Arkmedic discussed, another paper discovered that the spike protein was highly genotoxic and did in fact enter the nucleus. As these findings were extremely damning to the NIH, the leadership chose to address this issue by forcing the paper to be retracted for spurious reasons (a pattern that has sadly become quite common in the pandemic whenever inconvenient data emerges and may make these officials criminally liable for the catastrophic side effects that have resulted from their conduct).
In summary, there was a catastrophic failure on the regulator's part to not require genotoxicity for the COVID-19 vaccines (which may explain why the CDC has quitely removed the claim that their vaccines cannot alter your DNA). For those wishing to understand the potential genotoxicity of the mRNA vaccines in more detail, this recent paper by Peter McCullough and others provides an excellent summary of what is currently known on this topic.
A New Cancer Epidemic
For reasons detailed in the previous section, I had expected the mRNA vaccines to increase the rates of cancer in those who received them. However, what I did not expect was how rapid or unusual many of the cancers would be.
One of the most definitive cases I saw for the vaccine’s causing cancer was shared with me by a friend and colleague:
I had a patient that was a late 20s male with no past medical history except for stable lipomas (benign fatty lumps under the skin) he had had for years.
When the vaccine became available, he took both doses of Moderna. Shortly after the second dose, his previously stable lipomas started growing (this is extremely unusual). A month later, he was able to receive a biopsy for the lipoma and it was determined to be a very rare sarcoma.
The patient then full body imaging to stage it, cancer was also detected in the organ where this type of cancer is almost always found, he received a fairly invasive biopsy of that cancer and learned that it had the same genetic lineage as cancer found within the lipoma.
When I later looked up this cancer, I found out there are less than 100 cases a year of it in the United States, it never appears in that patient demographic, it never presents in this manner, and has a very poor prognosis.
Note: One of my good friends who is a nurse had a sarcoma form with a very similar progression in her husband following vaccination.
In general, I tended to observe that the cancers I heard of typically progressed rapidly, sometimes were quite unusual types, and often were (eventually fatal) recurrences of cancers that had gone into remission years before. Given that cancers normally take years to grow before they are large enough to even be detected (one estimate pegs it approximately ten years), the fact that I was seeing numerous immediately visible cancers emerging within months of vaccination was highly concerning.
In parallel, I also came across many cases of individuals rapidly developing diseases typically associated with immune suppression after vaccination. These cases were part of a project I began at the start of the vaccine rollout where after I began to have countless people contacting me sharing stories of severe or fatal reaction they observed following vaccination. After I realized almost none of my colleagues were open to listening to me, I decided at the very least I could verify and document these reports and then share them with the appropriate audiences. The tragic thing about this experience was that the cases I alone encountered had previously been sufficient to consider pulling a vaccine from the market. Unfortunately, like many other red flags, they were instead ignored. Within this compilation, the cases I encountered pertaining to the focus of this article are summarized under the section titled “Immune Suppression and Cancer”
Additionally, of the most common side effects of the vaccine has been the development of shingles, a complication that strongly indicates the vaccines suppress the innate immune system. One possible explanation for this phenomenon is the suppression of CD8 cells, immune cells responsible for both eliminating cancerous cells and suppressing shingles infections, which physicians such as Ryan Cole have observed significantly decline following COVID-19 vaccination.
All of these observations led me to suspect that the mRNA vaccines had a high propensity for creating genotoxicity in cells and also suppressing the immune response that would typically eliminate these cells. This hypothesis was further strengthened after the studies (detailed in the previous section) were published and provided strong evidence this could occur.
Typically, any time living organisms are exposed to a toxin or disease, reactions to the disease distribute on a bell curve resulting in the majority of them having relatively minor or invisible symptoms and only a small minority having significant side effects. Given that cancer is typically a slowly progressing disease, my great fear is that the rapid cases of cancer we have seen thus far are the outliers that represent the tip of the iceberg, and a significantly greater number of more slowly progressing cancers will emerge in the future.

Or as Jill Biden stated to Newsmax this week:
“I think in the next couple of months you’re going to see more cancers,” added the first lady. “It’s not a red issue, a blue issue,” Jill Biden added. “Cancer affects every American.”
Her rationale for this trend was people finally going back to doctors and getting caught up on their cancer screening, which is odd, given that the pause in seeing doctors for non-essential visits ended over a year ago.
The Cancer Vaccine?
Are you upset that cancers are on the rise?
Well, I have great news for you!
Moderna, another Covid vaccine company, is now working on a “personalized cancer vaccine”. (I guess they do not yet consider their Covid vaccine to be a “cancer vaccine”). So, since Covid vaccine sales are flatlining, they are now looking to create a new revenue stream with “personalized cancer vaccines”! Those for sure will work great, right? For sure, desperate cancer patients will be good for cash generation — and the market may be huge!
Will the FDA approve those “cancer vaccines” based on results in a dozen mice? Would you recommend a “personalized cancer vaccine” to your personal friends?


Comments
Post a Comment