if you don't like the data, stop reporting it? ONS edition
if you don't like the data, stop reporting it? ONS edition
there has been a worrying trend of data series being eliminated by health agencies when they trend against covid vaccines. it's time we demanded to know why.
the ostensible purpose of public agencies is to serve the public.
but how is the public served by selective data use and outright data suppression?
it’s enough to make one wonder about precisely for whom these purported public servants work. the CDC took its system offline for months in the middle of what remains a “declared emergency” to do an “update.” i struggle to see the sound or needful basis for so doing.
the ONS in the UK has been playing many of the same games and engaging in quite a lot of “hide the ball” besides. that said, they are still the only agency i know of that was reporting covid and all cause deaths by detailed vaccine status that allowed us to see not just the bayesian rig job of only counting “full vaccinated +14-21 days” and so i continue to focus on their data for despite all the apparent issues, definitions of covid death, and seeming undercounting of the unvaccinated (many of which have been so ably laid out by gatopals™ norman fenton and martin neil, see footnotes 6-11 HERE) it allows for some analyses that no other sets do.
my goal is so doing is to show that even when accepting this slanted playing field and steel-manning the case for vaccine efficacy on all cause mortality, they still fail badly. whether vaccines ever worked in this regard could be debated, but if ever they did, they certainly do not appear to anymore and that trend looked to be worsening in may of 2022 when the ONS (yet again) terminated a data series where the problems with the jabs were getting too bad to hide.
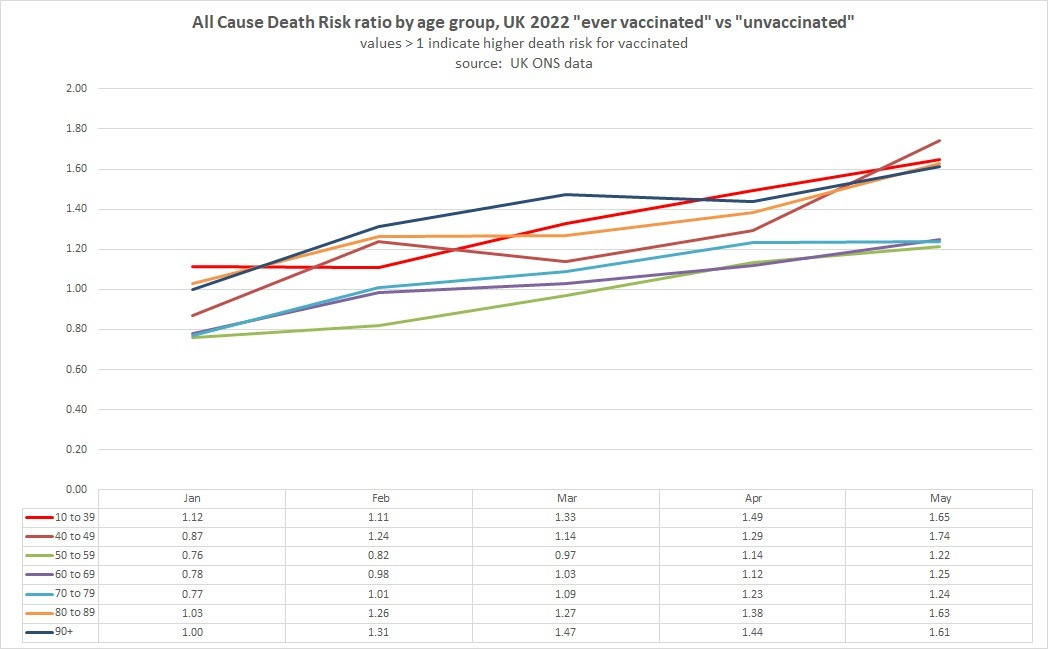
(you can see this full analysis HERE and another slice at the same issue using the ONS’s own ASMR calculations and nothing else HERE)
what makes this question so poignant is what was happening right when this series was terminated. because here is something quite curious, no?
ONS ended reporting of the deaths by vaxx status series in may.
the june all cause mortality numbers positively blew out.
what had been a bit of a rise in may became a serious and persistent spike, especially in males and especially from 25-64.
this is an extremely unexpected result. post a pandemic like this one would expect big drops in all cause mortality (ACM) from “pull forward” and if you examine the 50+ groups that were basically all the covid deaths, you can see just that. april and a bit of may 2020 were bad spikes but then early 2021 showed a big drop. this is consistent with the “dry tinder” thesis of “the highly vulnerable died a bit early and their later absence led to lower deaths.”
but now look at the middle of 2021. deaths start to pick up in the non-culled younger cohorts. many had been wont to ascribe that to covid, but this seems an unsatisfying explanation as the variants then were known to be quite a lot milder and this seems an odd issue to suddenly slant young. it sure does line up with the period shortly after many of the young got vaccinated though. this is obviously not dispositive, but it’s hardly a “coincidence” to ignore either.
then 2022 hit and covid jumped serotypes to the highly differentiated omicron variants.
and by mid 2022, all cause deaths were exploding. the huge surge seems to align quite tightly with the spread of BA.4 as a major variant and the rise to dominance of later variants of similar genotype.
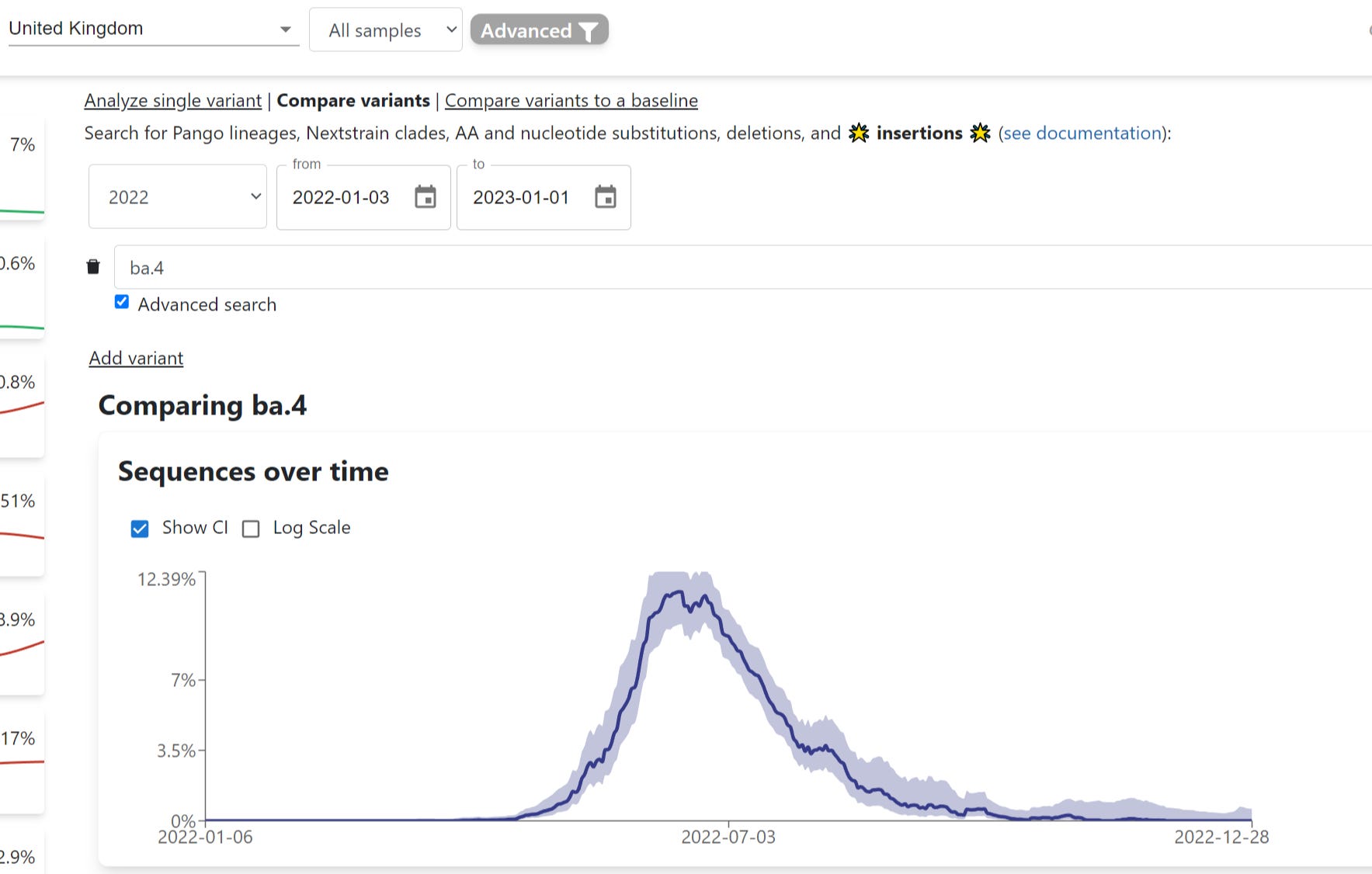
and this 2022 excess mortality surge did not align with “more covid deaths”
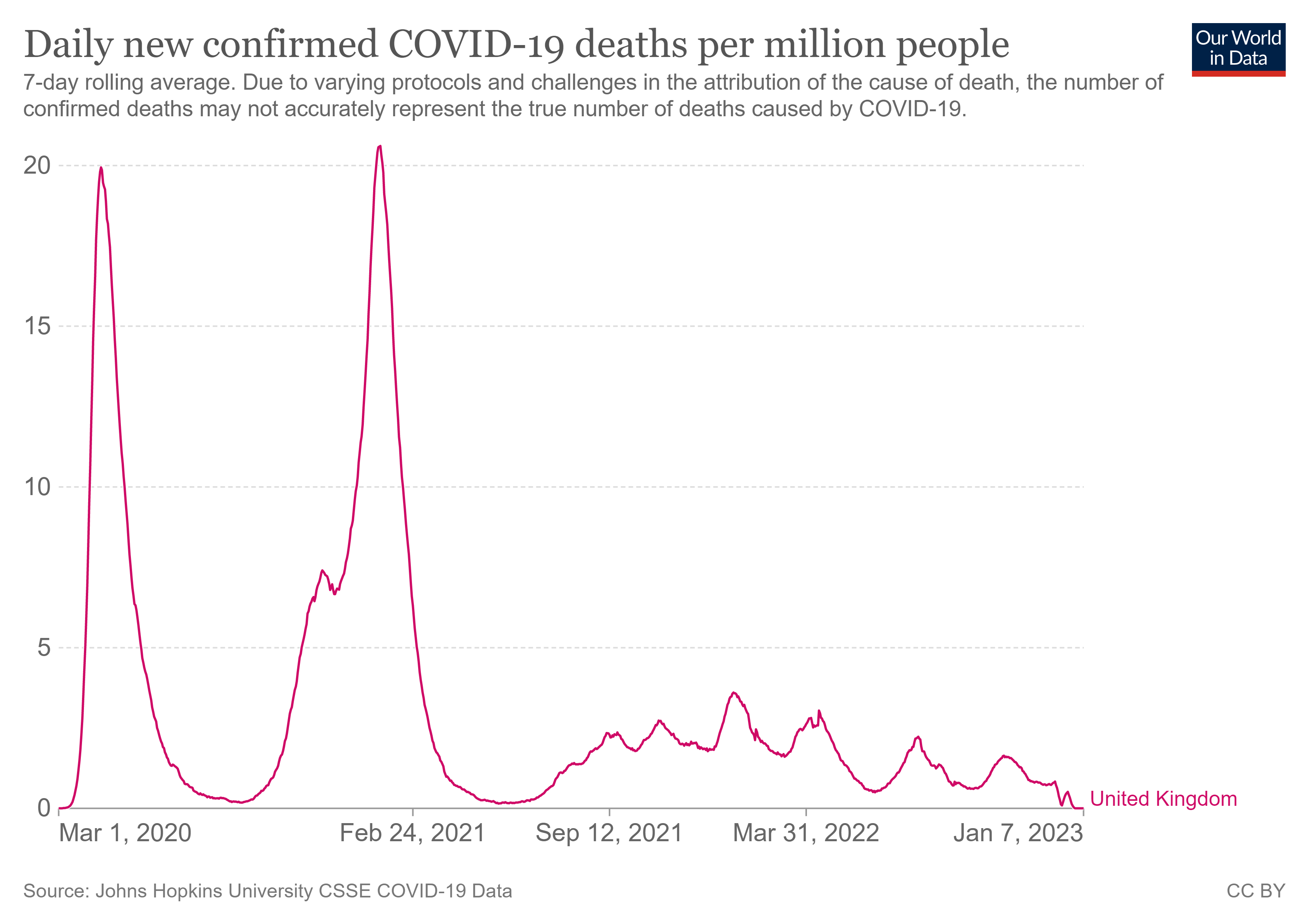
so it would seem that we might be looking for a different culprit here…
it sure would have been interesting to see what this did to the ACM relative risk rates by vaccine status that were already looking so problematic.
i have a sneaking suspicion that it did not make them look any better for the vaccinated.
(and that if they had, they’d have been published)
it would also be highly illuminating to see the variance in cancer, heart issues, blood issues, etc by vaccine status. it would really help assess ongoing issues and seems a glaring omission from the public data sets.
leaky vaccines (vaccines that do not stop contraction, carriage, and contagion) drive viral evolution to become vaccine enabled. it’s why we do not use them. the covid vaccines are notorious for generating just the sort of antigenic fixation mediated hoskin’s effect/OAS that causes this.
and omi looks like it was the escape variant. it’s so differentiated as to constitute a second serotype. the really interesting question may well be “would it ever have become so prominent without the herd antigenic fixation created by widespread adoption of non-sterilizing vaccines?
omicron is not a descendant of delta but rather a serious throwback with quite a lot of genetic differentiation. this led certain internet felines to ask some questions

because it sure looks like they were.
and it sure looks like this trend was highly variant driven. the ONS used to publish a wonderful series on per capita case rates by vaccination status. they played a bit of “hide the ball” with it by only reporting it as an aggregate since covid began, but it was easy to slice that into months by the simple expedient of taking the total through march and subtracting the total through february from it etc. et voila, we get this:
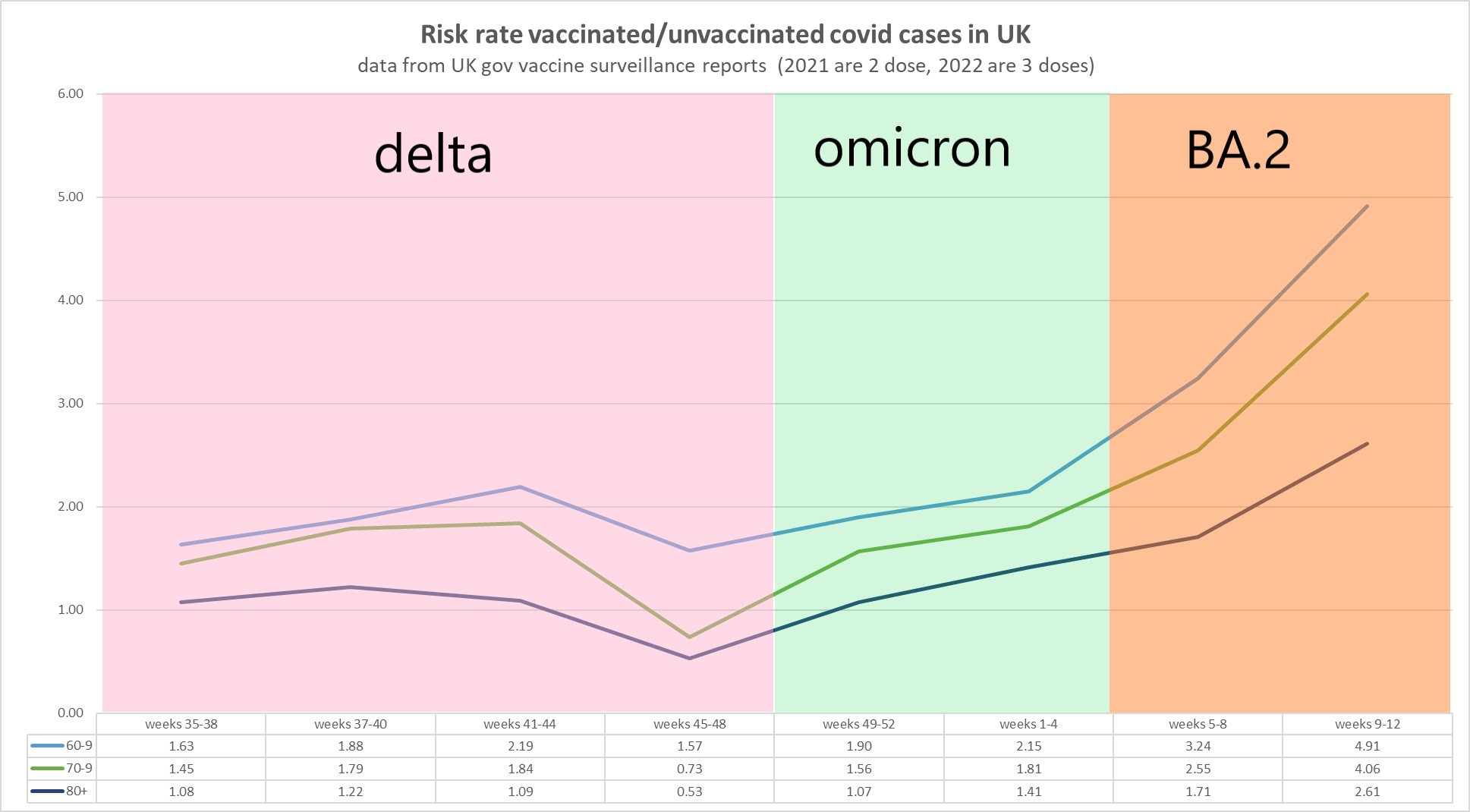
even as they moved to counting 3 doses instead of 2, relative risk blew out and was soaring into the 4’s for most age groups (data, links, methods HERE).
one can see the way the inflections track variant shifts and this is precisely what would be predicted in terms of viral evolution driven by leaky vaccines.
then, oddly, they stopped reporting the series post march. just as it was inflecting badly against vaccines.
one starts to wonder if there is a pattern here…
as it always seems both fair and right to give people an opportunity to explain and such information is never a bad thing even if you do not wind up agreeing with it. i am grateful to sarah caul (MBE. Head of Mortality Analysis @ONS), who was kind enough to provide some answers.
(this sort of access to people/networking constitutes the truly irreplaceable aspect of twitter)
for the record, i never referred to her or anyone as evil in this conversation. that was a straw man injected by another commenter who was seeking to tag sarah in on the discussion.
our dialogue went like this.

i have not, as of this writing, received a response to that last question but will make an effort to see if i can do so because i’m struggling to see the case to be made here.
to be sure, the past data relies on a dated census that was likely making “unvaccinated” look like too small a group because they were taking “the number of people vaccinated” and subtracting it from “population” to get there and so if population is too low, unvaxxed will look too small and thus vaccine efficacy will appear greater than it is because the base-rate death per capita will be spread across too few people.
but if this was “good enough to make pro-vaccine claims in early 2022” i’m a bit puzzled as to why it is suddenly no longer up to the task and why this new failing aligned so precisely with the moment that the all cause deaths figures spiked and likely would have swamped any slant.
this is especially provocative as it’s at least the second time they have done this with important data right as it turned sharply.
“we thought no information was better than some right at the moment of inflection when such information was most needed to make life altering decisions” seems quite a call to make.
one might think it would warrant greater explication than “we went dark for 8 months to have a think about how to make it better.”
i’d love to get one.
(note: please do not pick on, harass, or swamp sarah or other ONS folks here. she has been engaging in dialogue, this is probably not her call anyhow, and i REALLY do not wanna be “that cat” who sics hordes of angry people on folks instead of talking to them and who, as a result, nobody feels like they can have a sane or frank conversation with. let’s keep access open by being respectful and stand as the side of discourse not demagoguery and mob behavior)
this same trend has been much in evidence from canada and australia to the CDC who infamously stopped reporting all manner of all causes deaths for months on end to do “system maintenance” in the middle of a declared emergency. what they brought back online raised more questions than it answered.
most agencies will not even report all cause mortality by vaccine status at all, much less in a format that allows you to measure it from jab one and not from “last jab +14 or +21” which can be so badly misleading.
it’s honestly incredibly jarring when you actually step back and see the totality:
during the most allegedly dangerous pandemic in decades in which countless rushed and high-cost “mitigations” from lockdowns to distancing to travel bans to masking and warped speed vaccines with never before approved in humans methods of action, the agencies who have the information needed to assess the efficacy of these interventions have been systematically suppressing and slanting the data.
they have made claim after claim about safety, efficacy, and protection and cast as moral duty and social benefit what may well inflict severe public harm and represent the worst cost/benefit trade offs in the history of public health.
the time for “hide the ball” is over.
the time to stomach not being allowed to see what is going on is over.
given all we have seen and imputed, the time in which benefit of the doubt may be countenanced much less deferentially granted is over.
agencies that will not release complete, raw, auditable, and untainted data to allow for widespread independent analysis are simply no longer worthy of trust.
what else can one say about those who bury the information needed to establish the “informed” part of “informed consent”?
their silence and censorious natures stands as indictment that they do not serve the public and can any really doubt that if the full data validated their ends and narratives that they would not be trumpeting it from the ramparts rather than cloistering it close?
the time for the tolerance of these cut-rate wizards and the tatterdemalion curtains behind which they hide is over.
public health runs on public trust.
and if they won’t trust us, why on earth should we trust them?


Comments
Post a Comment