A Case Study in Covid-19 Vaccine Related Death Certificate Fraud
A Case Study in Covid-19 Vaccine Related Death Certificate Fraud
This is how fake science works. The answer you do not like must bring unassailable proof. The answer you prefer does not have to provide any evidence whatsoever, and is true until proven otherwise
While graphs and statistics run by no-skin-in-the-game amateurs can offer insights, they may lack the context and nuance necessary for informed decision-making, particularly in complex systems such as exist in our aggregations of national medical diagnostic data.
This is how fake science works. The answer you do not like must bring unassailable proof. The answer you prefer does not have to provide any evidence whatsoever, and is true until proven otherwise (wink-wink, nudge-nudge).
As previously mentioned on X, and as many of my readers are aware, since January 2023, I have experienced the loss of nine family members (Aunt/Uncle/First Cousin or closer). These losses, all associated with or caused by cancer, occurred among individuals aged 70 and above. Among them, all nine were Covid-19 mRNA vaccinated and boosted, two were undergoing stroke rehabilitation, and in one instance, the cancer had been in remission for a decade. However, to provide context, over the past 60 years, that same family grouping (factoring in generational turnover) has only encountered three cases of cancer, with just one resulting in death after a prolonged battle (prostate cancer). Cardiovascular and heart diseases have been more of the key issue inside our lineages.
Out of a family group totaling approximately 105 individuals, this occurrence (8.6%) represents a significant deviation from the norm for deaths alone, not to mention all those deaths being from cancer alone. Even factoring in the average age of those affected, this equates to a 30 to 50-sigma event for our family group. Throughout 2023, my wife and I dedicated a considerable portion of our time to either working or attending funerals.
An Aggressive Second Cancer in a Single Year
In December of 2023, we tragically lost one of our close family members to colon cancer. The journey began when she noticed a sizable and rapidly growing lump in her lower left quadrant in early September of the same year. She had just recovered from her successful breast cancer surgery a mere eight months prior. This lump caused discomfort, particularly during peristalsis of the large intestine passing through her descending colon. Consequently, she promptly scheduled an appointment with her general practitioner.
My wife and I accompanied her to several appointments with both her general practitioner and cancer-hematologist throughout October and November. By November however, the lump had rapidly grown to the size of a grapefruit, causing her significant pain. The medical team responded promptly, administering appropriate pain relief and conducting various tests, scans, and treatments for colon cancer. I applaud her entire compassionate and responsive set of care givers.
I met with the general practitioner face to face on October 13th 2023, and the following discussion ensued.
TES: “Thanks for the extra attention here with us today Doc. She is adamant that her sudden onset arthritis, anemia, skin lesions, blistering, joint pain, bruising in her extremities, and now second cancer inside 10 months, are all a result of the Covid-19 vaccine. Do you think that these, are at least in part, due to the Covid vaccine?
Dr. GP: “Yes, I believe so. The change in state from prior to after was very stark. Plus I have seen this in other patients. She and I had this discussion on her last visit. She asked if all this, and her previous cancer, was from the vaccine, and I told her ‘yes’, or ‘most likely’.”
TES: “Will you diagnose this as cancer, and as Covid-19 vaccine injury in her medical record?”
Dr. GP: “I don’t have proof of either. I can cite her anemia, but we need more testing to prove a case and type of colon cancer. Let’s go ahead and get that scheduled.”
TES: ” Excellent doc, thanks. But it is, to your best judgment, colon cancer?”
Dr. GP: “Oh yes.”
We were directed by the general practitioner to a hematologist-oncologist for further evaluation. The initial Carcinoembryonic Antigen (CEA) measurement of 11.9 was indeed elevated, prompting concern. However, the hematologist emphasized that while an elevated CEA can suggest the presence of cancer, it is not definitive on its own. I highlighted to the specialist that time was of the essence, given that the cancer had gone from inception to grapefruit in size in a mere 90 days, and especially considering the ongoing treatment provided by both her primary physicians and the palliative care team, all operated under the assumption of a cancer diagnosis. Despite the lack of a definitive diagnosis, the urgency of the situation was clear, underscoring the need for prompt and decisive testing.
Despite our efforts to schedule appointments for further testing, her declining physical condition made it logistically challenging. Tragically, she passed away 107 days into her second battle with cancer in less than a year. The first instance, breast cancer, had been surgically removed in late 2022. Following her passing, I reached out to the hematologist-oncologist to inquire about her diagnosis in the medical records. His response was disheartening: “We had no proof. I can only give a cancer diagnosis based upon definitive evidence.” While this made sense, nonetheless the conversation underscored the frustration and sense of helplessness we experienced in the face of a disease that eluded clear diagnosis until it was tragically too late.
We were met with similar frustration, by a coroner’s office who was backlogged three months, and medical services who were wholly unprepared or unwilling to conduct a post-mortem biopsy to prove our case. We held a celebration of life for family and friends, and moved on sadly with our death-interrupted lives.
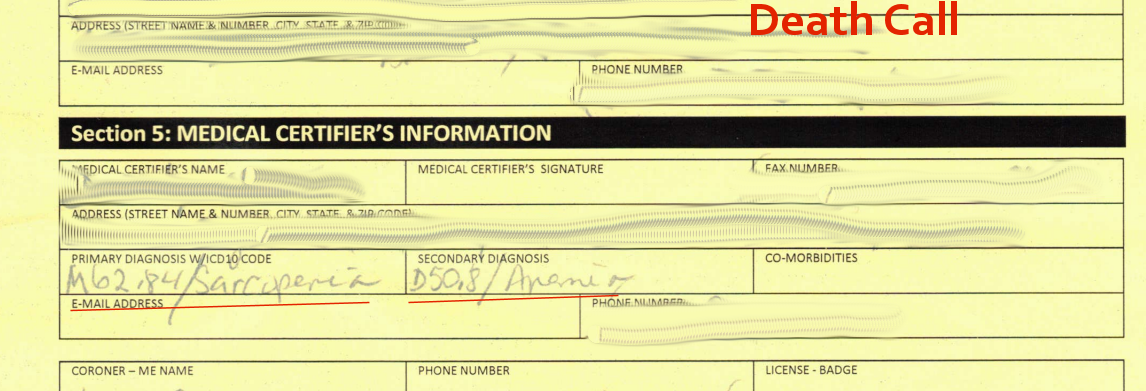
The Fraud
When the death certificate arrived this week from the state, as crafted by the hospice palliative care physician (who had never even seen her – remember, these people determine the greatest preponderance of ’cause of death’ calls), the Immediate and Underlying (and a fortiori Multiple) Cause of Death only had one ICD code listed: “Alzheimer’s Disease”. The malady was not even titled correctly: G30 (Alzheimer disease). Apparently, for a cancer diagnosis one must bring definitive proof, but for an ad hoc explanation one does not need proof at all, nay even a hint. You just merely fabricate the answer your state medical board enforces.
She never had, nor was diagnosed with, nor was even suspected of having Alzheimer Disease. She was sharp minded and functional up until mere days before she died.
This is how fake science works. The answer you do not like must bring irrefutable proof. The answer you prefer does not have to provide any evidence whatsoever, and is true until proven otherwise (wink-wink, nudge-nudge).
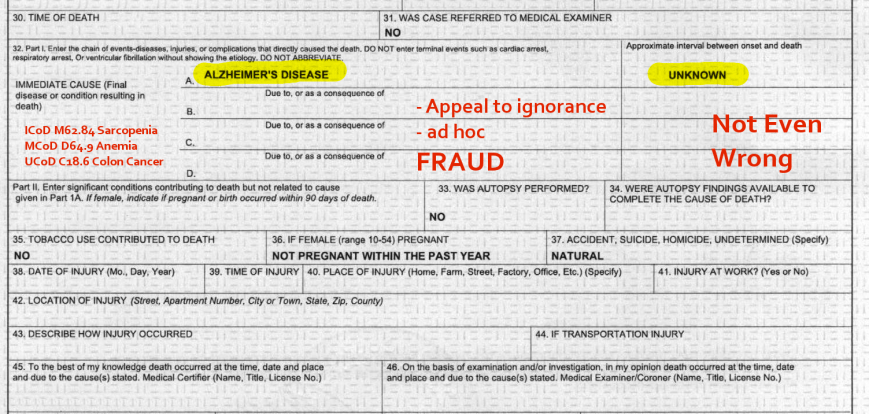
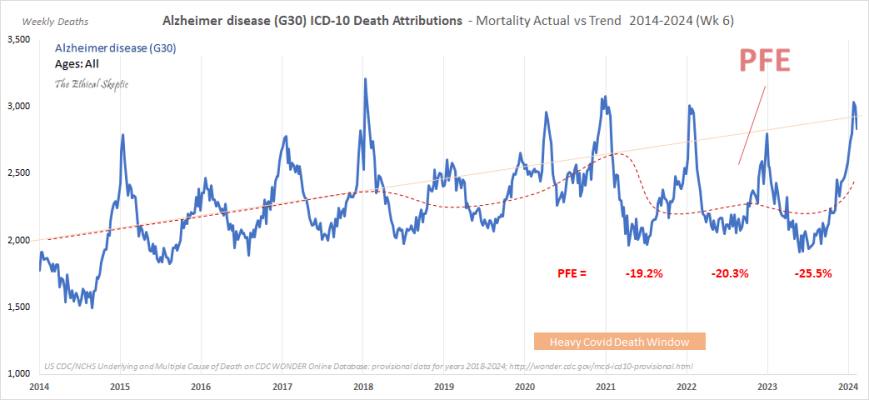
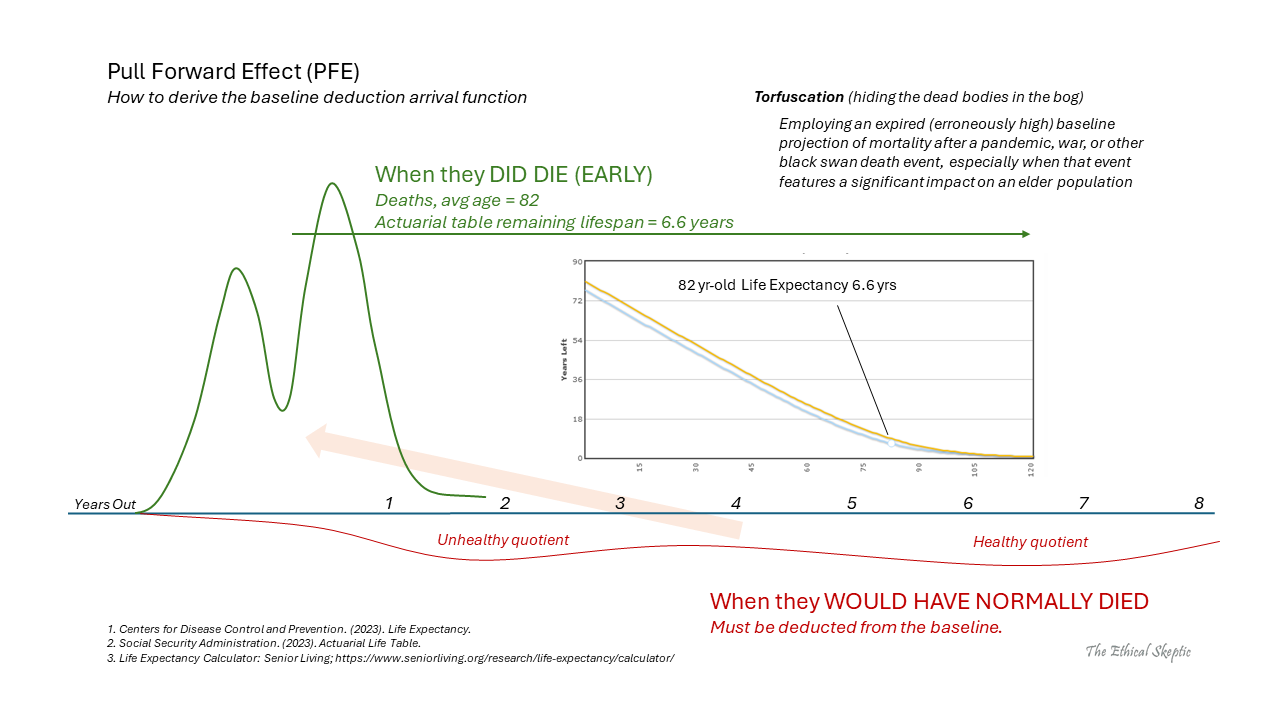
Here is why the state medical board and health department desired to convert a cancer death to “Alzheimer’s Disease” in particular. This was no accident, as there exists plenty of room for torfuscation (hiding the dead bodies in the bog) using the Alzheimer Disease ICD Code. There is room for 900 cancer deaths per week in the US which can be hidden inside this categorization’s pull forward effect (PFE) – and that is exactly what these criminals are doing.
This is exactly why they have tasked paid shills to attack me for having defined Pull Forward Effect in the first place. It is their secret recourse.
Alzheimer’s, my ass.
Indeed, this experience highlights the limitations of relying solely on raw data outputs, such as those provided by databases like the CDC’s Wonder. While graphs and statistics run by no-skin-in-the-game amateurs can offer insights, they may lack the context and nuance necessary for informed decision-making, particularly in complex systems such as exist in our aggregations of national medical diagnostic data.
Instead, it’s essential to look for signals that provide meaningful and actionable information, going beyond mere data aggregation. This requires a discerning approach that considers the broader context, including well established confounding factors and the limitations of available evidence. By prioritizing quality over the pro forma and seeking out meaningful signals, we can make more informed and effective decisions, especially in critical matters such as healthcare inside the Covid-19 post-pandemic crisis currently upon us.
Source: The Ethical Skeptic


{kind=link}
{kind=link}
Comments
Post a Comment