Estimating Vaccine-Induced Mortality, Part II: Isolating the Variable
Estimating Vaccine-Induced Mortality, Part II: Isolating the Variable
The Chloroquine Wars Part LIII
In Part I, I examined the first 30 days of vaccination programs throughout Europe, showing an estimated 1018 deaths per million doses (not even people---doses) of COVID-19 vaccines administered, judging by excess deaths compared to a starting baseline based on case fatality rates (CFRs). After a quick, but seemingly reasonable adjustment, I estimated 200 to 500 deaths per million doses delivered---based solely on deaths seemingly categorized as COVID-19 deaths. This would suggest, based on 4 billion doses already administered throughout the world, that 800,000 to 2,000,000 of the COVID-19 deaths recorded are actually vaccine-induced deaths. This does not even include vaccine-induced deaths that have not been recorded as COVID cases, though I suspect that latter number is smaller since the only good way to hide the vaccine mortality signal is to smuggle deaths through the already-established COVID death toll.

Can We Corroborate the Estimates?
As a quick observation, Norway reported 23 deaths at a time when 40,000 Norwegians had been vaccinated. Forgetting about the possibility of underreporting (including lagged reporting at that moment), this total represents 575 deaths per million doses administered. When Norwegian health officials finished assessing the first thirteen of these deaths, all of them were determined to be linked to the vaccines. Meanwhile, erstwhile health authorities in the U.S. continue to behave as if examination of the bodies is completely unnecessary [for their purposes].
More generally, we would like to find some way to isolate the variable that is the vaccines so that we can examine those effects outside of the context of COVID deaths. If health authorities can wash those numbers together, we can never know what the effect size of the vaccines looks like.
Nations around the world have been affected in substantially different ways by the pandemic. Those differences sometimes manifest in ways that allow us rare glimpses into the effects of variables. Natural experiments allow us to gauge the results. In particular, a closer look at nations that were left largely untouched by the pandemic (in mortality terms, at the least), gives us the chance to look for data consistent with the theory that vaccine-induced mortality is quite high during the experimental mass vaccination campaign.
While researching data related to vaccine-induced mortality, one of the best data-minds I know emailed me,
Has any country that you're aware of had substantial vaccine uptake without substantial covid? E.g., New Zealand or Australia should in theory make excellent "control" cases for the impacts of the vaccines sans covid -- except that they still have very low vax rates. (Sadly explainable equally well by: They haven't been scared enough by covid to get the vaccines out; or: they don't want a visible control case like that.)
I had already made a couple of observations about such nations, such as Cambodia, which has 1442 COVID deaths as of earlier this week---every one since the start of the vaccination program---but was spurred to perform a more exhaustive search. Hopefully, I did not miss any. Colored in the map below are the candidate nations. I tossed out the island nations (dark grey) because their results have been so distinctly different from those of the continental world throughout the pandemic. I tossed out nations in red due to substantial distrust of the data. The nations in yellow have administered very small numbers of doses of the vaccines, and the pattern of dissemination may be quite different than for largely wealthier nations that can organize programs targeting the highest at-risk first.
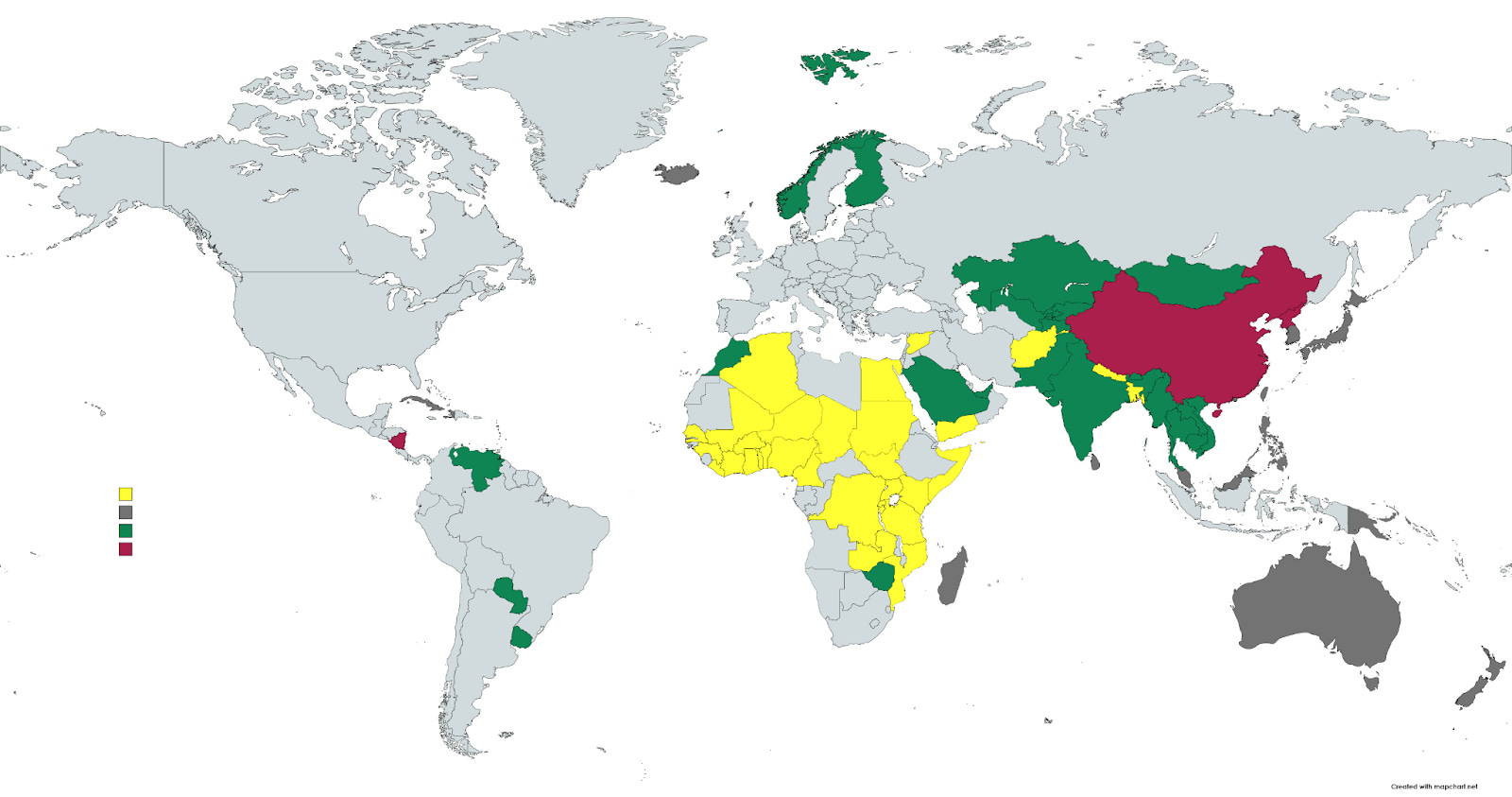
We are left with 23 (green) nations (rounding up for little Gibraltar), which house 1.88 billion people, which is roughly a quarter of the world's population. If I missed an interesting case, please let me know in the comments. I am happy to run the numbers with additional inclusions, where reasonable.
Here are there collective (official) statistics prior to the start of COVID-19 vaccine campaigns:
38.45 million COVID cases
529,228 COVID deaths
103.2 COVID deaths per million population
A total of 5 of these nations had more than 200 deaths per million
A total of 7 of these nations had fewer than 10 deaths per million
These nations spent an average of 332 days in pandemic prior to vaccination, and through August 1, 2021, were 168 days from the start of vaccination campaigns. Some vaccination statistics through August 1:
25.35% of residents in these nations have been vaccinated
10.36% have been fully vaccinated
673 million doses have been administered
Now, I'm going to save you the nitty gritty details of my current spreadsheet, but it looks something like this, and I just realized that I rounded some numbers for Cambodia and Laos before deciding to go big and automating the process better. Any changes are thus rounding errors of rounding errors (literally).
Understand that I do take these results with a grain of salt. This is what I'm happy to call a "first order analysis". But if you squint closely, you'll notice that adjusted (excess) deaths per million vaccine doses delivered is 411, which is slightly to the high side of the 200 to 500 range I roughly estimated from European data. Intriguing!
Here are some interesting observations:
Aggregate CFR was 1.48% before vaccination and 1.48% since vaccination began, though this result was highly variable by nation.
The number of COVID deaths per day was 3.82 as high since vaccination started as prior, while new cases were 3.80 as high. Morocco and Saudi Arabia were the only two nations in these groups to see lower average COVID death tolls since the outset of vaccination.
If deaths were scaled by 3.82 due to the vaccines, then there were 276,465 excess deaths during this time span.
India dominates these numbers a bit, so we'll remove India (and some other nations) and take another look or two, but first I'd like to check for a trend in (log scale) deaths versus proportion of residents vaccinated (ignore that Gibraltar has more vaccinated residents than residents...every culture has their kink, I guess).
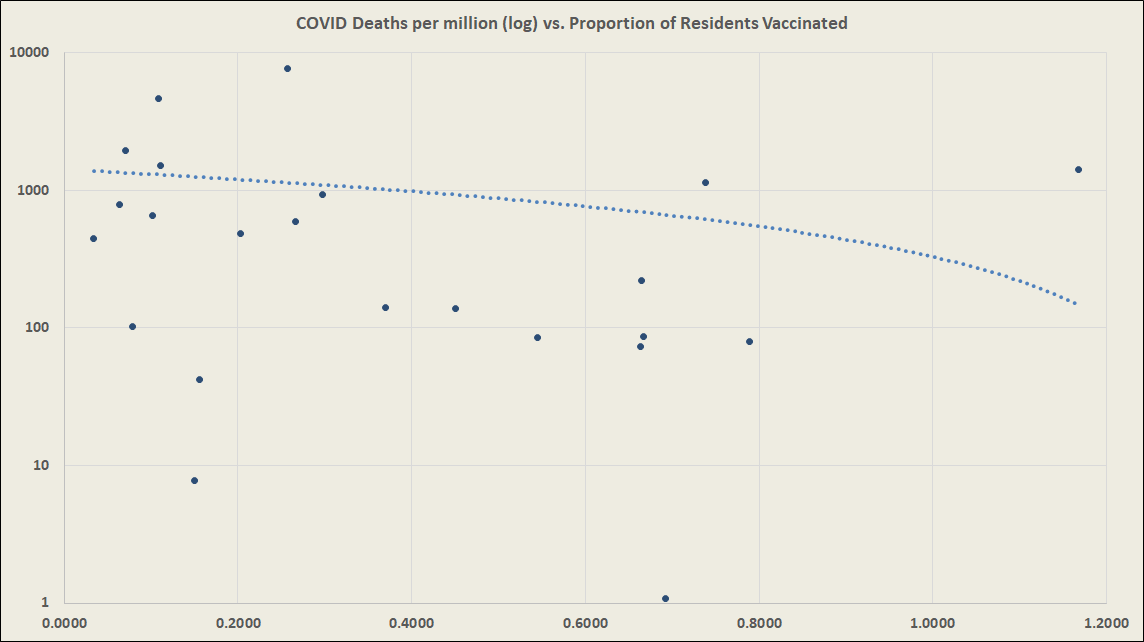
The outliers are Gibraltar in the upper-right, then Laos, Tajikistan, and Uzbekistan in the lower-left, and Paraguay up top.
If you're not used to seeing trend "lines" hook, that's just the compression of the logarithmic scaling of deaths per million doses administered (first or second). If we can assume that those at high risk---predominantly the elderly---are vaccinated first (or in a ring vaccination program), this trendline is highly consistent with the hypothesis that vaccination-induced mortality correlates highly with the same population most at risk for COVID.
Notice that during the first 30 days of vaccination in Europe, around 2.5% of Europe's population was vaccinated resulting in my estimated 1,018 deaths per million doses administered, which falls just under the start of our trendline.
The removal of India has the following effects:
Post-vaccination CFR jumps to 2.24% while pre-vaccination CFR gets slightly larger (1.61%).
The scaling factor for daily COVID deaths jumps to 4.35, meaning the 22 nations see 335% more COVID deaths since vaccination began.
The number of excess deaths per million doses drops a bit to 363, quite in the middle of the range we established from the European data set.
Now, let's remove all nations that had more than 100 deaths per million prior to vaccination programs to zoom in on the nations that had been most untouched by the pandemic. These remaining 13 nations have a combined population of over 354 million, and their populations have received a similar number of doses to the original cohort of which they are a subset. Weirdly, due to the UAE, there are more second doses than first doses.

We see,
The adjusted number of excess deaths per million doses is 318, which is a little lower than for the full group, but still well without our previous range (200 to 500) of expectation based on the hypothesis that the vaccines are killing people.
The COVID deaths per day have been 11.61 times as high for these nations as prior to the outset of vaccination!
In all, 5 of these 13 nations have seen over 90% of their COVID-19 fatalities since the outset of vaccination programs. Only Uzbekistan has seen less than 48.5% of its COVID-19 deaths since the start of its vaccination program
I am modeling in some additional deaths as internally consistent proportions (national CFR) for ongoing cases, which alters the mortality numbers slightly. To this point in the pandemic, modeling the lagging cases has shown consistent enough success in models that I'm comfortable thinking it improves the analysis. Leaving it out would require us to shorten our window of analysis.
Additional Observations and Questions
On face, these results reinforce the case that the experimental vaccines are killing people. At the very least, this is one more dramatical [lack of] safety signal that should spur authorities who care about our health to come to the table for a discussion about how to refine the data they're not analyzing to anyone's knowledge.
One worry an observer might have with this analysis is seasonality effects. However, 22 of the 23 nations on the list have been vaccinated for four to seven months with seasonality (assuming two waves per year) seemingly intact.
More concerning is that numerous of these nations---largely located in Asia---seemed to have no susceptibility at all to the pandemic prior to vaccination. There are a lot of theories as to why this might be aside from just vaccines triggering deaths.
Might PCR testing pick up signals from attenuated virus vaccines, resulting in case explosions (from almost none) to match the [new] deaths?
Could some of these vaccines have faulty production such as in the Cutter incident during polio vaccine rollout? This could result in cases and deaths?
Paraguay has by far the greatest signal of vaccine-induced mortality. It stands out as one of the only nations on Earth to use both Chinese and also Western vaccines. Is there any reason such a combination could result in more volatile disease spread?
Do we really believe that the braintrust at the FDA and CDC are entirely unaware of these observations?
Meanwhile, health authorities still seem to have no issue with the lack of risk report or risk-benefit analysis performed by any of the vaccine manufacturers or anyone else. This strikes me as one of the worst signs in my lifetime that corporations have taken over government on an essentially complete level.


Comments
Post a Comment