Covid Vaccines: A Reality Check
Covid Vaccines: A Reality Check

Published: December 28, 2021
Share on: / /
The latest unbiased facts on covid vaccine safety and effectiveness.
Covid vaccine effectiveness
Prior to the most recent immune-evasive mutation (omicron), covid vaccine protection against infection and transmission decreased to zero within about half a year, whereas protection against severe disease and death in senior citizens decreased from about 95% to about 50% within 6 to 9 months (depending on the vaccine, see chart below).
Against omicron, protection against symptomatic infection has been shortened to just a few weeks, while protection against severe disease remains uncertain. However, there are indications that omicron really is significantly milder than previous variants, even in people without prior infection. Otherwise, omicron would have posed a major challenge to the entire global vaccination campaign.
Studies that claimed more durable vaccine protection typically combined several time frames (e.g. January to August instead of just August) or age groups (vaccine protection is more durable in younger people, but their covid risk is also much lower). An example of the latter is the Qatar study, the participants of which had a median age of just 31 years; in participants older than 60, protection against severe disease had fallen to 60% within 7 months (only shown in the study annex).
Vaccine protection against infection and severe disease (all age groups):

During 2021, covid vaccines may have saved several hundred thousand lives by mitigating the impact of the covid waves in spring (Alpha), summer (Delta) and early winter (also Delta). This can easily be seen by comparing countries with a high vaccination rate to countries with a low vaccination rate (e.g. Western Europe to Eastern Europe), or by comparing the impact of covid waves before and after vaccination in countries with a high vaccination rate (see next chart).
Importantly, prior to the winter wave of 2021/22, only about 20% to 50% of people in Western Europe and most US states had developed natural (i.e. infection-acquired) immunity against covid. In Latin America, parts of Africa (including South Africa) and parts of Asia (e.g. India), about 50% to 80% had developed natural immunity against covid. In some of these places, the flu has already returned.
Much lower covid deaths in high-vaccination EU countries:

Since autumn 2021, several countries reported a negative vaccine effectiveness against infection, that is, vaccinated people had a higher infection rate than unvaccinated people. In countries like the UK, raw negative vaccine effectiveness reached up to minus 100% in some age groups (i.e. vaccinated people had double the infection rate compared to unvaccinated people; see next chart). In response, several countries simply stopped publishing this data.
The most likely explanation for this observation is a catch-up effect: for several months after vaccination, vaccinated people had a lower infection rate than unvaccinated people. As a result, there are more “recovered” people – which have the strongest and most durable protection – among the unvaccinated than among the vaccinated. Once vaccine protection has declined, infections among vaccinated people simply catch up.
A more troubling explanation for negative vaccine effectiveness against infection, proposed by some skeptics, would be some kind of negative immune effect. For instance, it is known that covid vaccination can cause a temporary immune suppression (lymphocytopenia) that can last for up to a week and possibly longer, and that likely plays a role in the well-documented post-vaccination spike in coronavirus infections. It is also known that vaccinated people, once infected, develop only a partial immune response, which might increase their risk of re-infection.
However, data from the UK and elsewhere shows that a vaccine booster dose temporarily restores vaccine protection against infection, although again only for a few months, or even just a few weeks against the immune-evasive omicron variant (see chart below). Nevertheless, this temporarily restored protection appears to support the “catch-up hypothesis”.
Claims of negative vaccine effectiveness against severe disease and death (i.e. covid vaccines making covid worse), promoted by some hardcore vaccine skeptics, have currently no basis in reality (they were based on statistical effects and age-group differences).
However, such a negative effectiveness, which would point to antibody-dependent disease enhancement (ADE) or negative antigenic priming (OAS), cannot be totally ruled out against future coronavirus variants, due to the short-term nature of covid vaccine trials.
UK: Negative vaccine effectiveness against infection:

Vaccine injuries
Covid vaccines have been shown to cause, in “rare cases”, severe and fatal cardiovascular, neurological, immunological and metabolic adverse events (see an updated overview of severe covid vaccine adverse events). More recently, covid vaccines have been associated with various auto-immune diseases, tumor growth and cancer, and new-onset diabetes and diabetic ketoacidosis.
The US VAERS system currently shows about 20,000 post-vaccination deaths, of which about 10,000 from the US itself. Previous studies showed that passive surveillance systems (like VAERS) capture only about 5% to 20% of adverse events, while a recent study found that about 80% of post-vaccination deaths reported to VAERS had plausibly been caused by covid vaccines.
Thus, it is conceivable that covid vaccines may already have caused, or triggered, about 100,000 deaths globally. The WHO VigiAccess database, which combines several national databases, currently shows about 3 million reported covid post-vaccination adverse events, of which about 85,000 severe adverse events and close to 20,000 deaths (more on excess mortality below).
Post-vaccination deaths reported to the US VAERS system:

Concerning heart inflammation (myocarditis and pericarditis), a recent comprehensive analysis by researchers at the University of Oxford found that in males between 16 and 39 years of age, the risk of myocarditis after vaccination was significantly higher than after coronavirus infection (see next chart). In particular, this was the case for the second and third dose of the Pfizer mRNA vaccine, the first and second dose of the high-dosed Moderna mRNA vaccine, and even the second dose of the AstraZeneca DNA vaccine.
Since covid vaccines provide no significant protection against long covid (which requires only a mild infection), one may conclude that for healthy and lean adolescents and adults below the age of 40, especially males, the risk/benefit ratio of covid vaccines looks rather unfavorable. Indeed, this is also the conclusion that a senior FDA executive appears to have reached during a recent hearing.
If subclinical cases of myocarditis are taken into account (which may also trigger a cardiac arrest, see below), the risk of myocarditis after two-dose mRNA vaccination in young males reaches about 1 in 1000, a figure confirmed by recent studies from Hong Kong and from Ontario. In this regard, Austrian pharmacology professor Dr. Hartmut Glossmann, one of the most cited Austrian scientists in the world, described covid vaccines as “the biggest drug scandal” he has ever witnessed.
Myocarditis after covid vaccination vs. infection in young males:

VAERS: myocarditis after covid vaccines (2021) and flu vaccines (all years):

Indeed, the issue of post-vaccination heart inflammation appears to be closely linked to the unprecedented increase in heart problems, sudden cardiac arrest and even sudden cardiac death observed in athletes during recent months. The online platform Good Sciencing has compiled a comprehensive list that includes already 384 athlete cardiac arrests and 223 athlete deaths, showing a strong increase since about May 2021. In recent weeks, several top players per week have been affected (see image at the top of this analysis).
From a medical perspective, there are two conceivable causes for this observation, a bad one and a worse one. The bad one is that most of these athletes had recently been vaccinated and had a subclinical (unnoticed) acute heart inflammation when they collapsed while exercising. The solution to this is to simply pause exercising for a few weeks after vaccination, which is indeed recommended in some countries (e.g. in Israel).
The more troubling explanation would be that many of these athletes had been vaccinated months ago and developed chronic heart damage that caused heart failure or sudden cardiac arrest during intensive exercise. Previous in-vitro and animal studies showed that the coronavirus spike protein alone, which is produced by covid vaccines, can severely damage heart muscle cells and endothelial cells (i.e. veins and arteries).
If this is the case, it is likely that many more people (i.e. non-athletes) may be affected by this issue and may develop acute heart problems or other cardiovascular issues later on (e.g. when exercising or simply climbing stairs). The solution to this would be to absolutely avoid intravenous vaccine injection, or to simply stop covid vaccinations in the general population altogether.
Athlete cardiac arrests – increase in 2021:

Already, several countries have stopped DNA adenovector vaccines (J&J, AstraZeneca) due to blood clotting issues, while several other countries stopped the high-dosed Moderna mRNA vaccine due to the increased risk of myocarditis in young people (especially males). Even the second dose of the Pfizer mRNA vaccine has been stopped for adolescent in some Asian countries.
The Canadian province of Quebec decided to stop booster vaccinations of senior citizens who had previously been infected after an increase in life-threatening booster vaccine reactions had been observed (previously also reported in Germany and in Israel). In general, it is known that covid vaccine-related risks increase with additional doses, and the mRNA lipid nano-particle technology itself is known to cause toxicity if injected repeatedly.
Concerning children younger than 12, several countries (e.g. Finland) decided against a general recommendation to vaccinate them, while some other countries (e.g. the USA) approved a low-dose Pfizer mRNA vaccine for this age group. By early December, about 5 million US children aged 5 to 11 had received a first dose of the Pfizer vaccine, which accounts for about 20% of children in this age group.
As a result, the US VAERS system shows several dozen reported cases of post-vaccination myocarditis, stroke, allergic reactions, neurological disorders, and even death in children aged 5 to 11 (see this compilation). Given under-reporting and reporting backlogs, the true figure of serious adverse events may already be in the hundreds.
Nevertheless, the CDC director recently argued that she has “not yet seen any safety signal”; previously, an FDA advisory committee member acknowledged that “we’re never going to learn about how safe this vaccine is [in children] unless we start giving it.”
Meanwhile, the risk of severe covid in children has turned out to be even lower than previously thought, as at least one fourth of US coronavirus-positive child deaths were shown to be entirely unrelated to covid. Indeed, in US male adolescents, there were about ten times more suicides than covid deaths in 2020.
Concerning post-vaccination miscarriages, still births and birth defects, there are several “anecdotal” reports of possibly vaccine-related incidents, especially concerning cardiac anomalies and pulmonary hemorrhage (bleeding lungs), but no statistical evidence yet. The US VAERS system currently counts about 3,300 post-vaccination miscarriages, and tens of thousands of British women have reported post-vaccination menstrual disorders.
In Scotland, an investigation has been launched to determine the cause of a significant increase in deaths of newborns during September. Besides the vaccination of pregnant women, a simultaneous RSV respiratory virus summer wave might also be a possible explanation.
Scotland: Increase in neonatal deaths in September:

Finally, several countries have recorded an unexplained excess mortality in the wake of covid mass vaccination campaigns. This was first noticed in Israel in the spring of 2021 (in parallel to a “murky wave of heart attacks”). Over the summer, Britain recorded several thousand non-covid excess deaths, mainly due to cardiovascular events. Moreover, Britain recorded excess deaths in adolescent males, but not females, in parallel to the vaccination campaign in this age group.
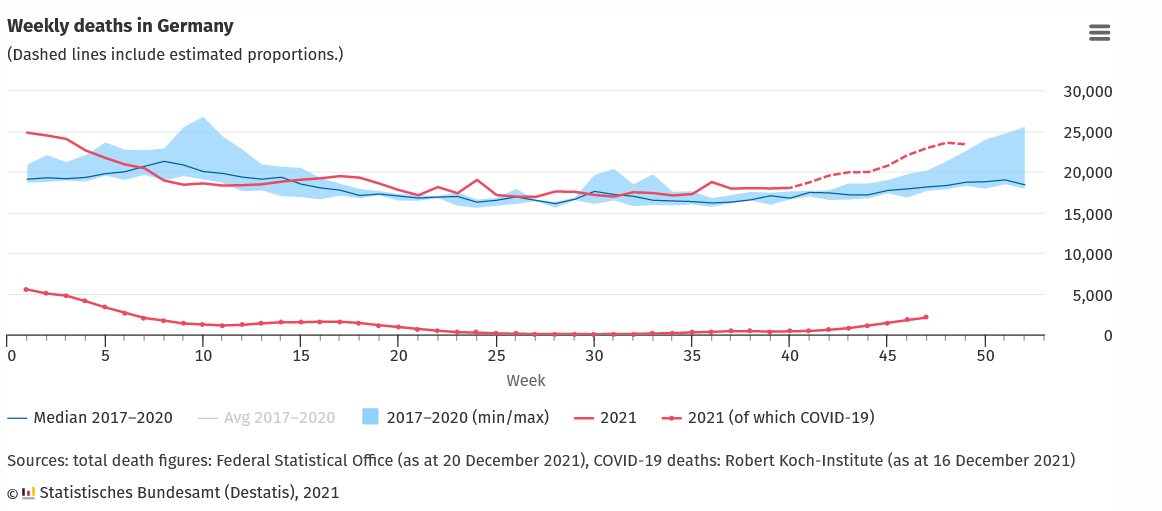
Since September, Germany has been recording an unexplained and unprecedented non-covid excess mortality of several thousand people. More recently, Spain has been reporting a similar unexplained excess mortality. In Switzerland, which is using mainly the high-dosed Moderna mRNA vaccine, a significant non-covid excess mortality has been recorded in parallel to the ongoing booster campaign.
(The Moderna vaccine has three times the mRNA dose of the Pfizer vaccine; thus, after three vaccinations, the total mRNA dose is nine times higher, without providing any substantial medical benefit. In medicine, the dose of a drug should never be higher than necessary.)
Nevertheless, this excess mortality effect is not observed in every country (e.g. not in Nordic countries) and may be due to factors other than vaccination (e.g. pandemic and lockdown-related effects). For instance, in the US, drug overdose deaths and teen suicides have reached record levels.
Germany: Unexplained non-covid excess mortality since September:
Britain: Excess deaths in teenage boys:

Vaccine passports
Since covid vaccines do not confer meaningful protection against infection and transmission, and the risk of severe covid is very low for large parts of the general population, “vaccine passports” and covid vaccine mandates have no medial or epidemiological justification.
Pressuring people to get vaccinated (e.g. through a “no jab, no job” scheme) must be seen as a major medical crime and a crime against humanity, especially given the superiority of natural immunity and well-documented vaccine-related health risks.
Instead, it appears likely that “vaccine passports” are being promoted primarily for strategic purposes, as a precursor to digital biometric identity and payment systems.
Conclusion
In 2021, covid vaccines likely saved several hundred thousand lives, but they may also have caused or triggered about 100,000 deaths and many more injuries globally.
The risk of covid vaccine injuries increases with additional booster doses, and several countries have already suspended various covid vaccines partially or completely.
Covid vaccine protection decreases substantially within about half a year and it collapsed against the immune-evasive, but apparently milder omicron variant.
For healthy and lean adults below 40 years of age, as well as for children and adolescents, the risk/benefit ratio of covid vaccination does not appear to be favorable.
“Vaccination passports” and covid vaccination mandates have no medial or epidemiological justification. Coercing people to get vaccinated must be seen as a crime against humanity.
Covid vaccine safety resources
- OpenVAERS (OpenVAERS)
- Athlete cardiac arrests (Good Sciencing)
- Child covid vaccine injuries (Rees/Assyria)
- Covid Vaccine Injuries (Telegram, 90k followers)
- Covid vaccine adverse events (SPR overview)
Video: Cardiac arrests in athletes
Video: Neurological vaccine adverse events (18+)
Postscript
1) Are covid vaccines part of a “global depopulation agenda”?
Some critics argue or suspect that covid vaccines may in fact be part of a global depopulation agenda, orchestrated by billionaires like Bill Gates in order to meet challenges posed by dwindling natural resources, climate change and the fourth industrial revolution.
Such a vaccine-related depopulation agenda could be achieved by either increasing global mortality (e.g. via heart disease) or by reducing global female (or male) fertility.
With regards to the former, if covid vaccines should turn out to dramatically increase the long-term risk of cardiovascular disease and heart failure, this could indeed increase global mortality, even in non-senior citizens.
With regards to the latter, it is true that technologies for “anti-fertility” vaccines exist (they produce antibodies against fertility-related hormones). Furthermore, there are credible reports – disputed, but not refuted – that in 2014, three biochemistry laboratories in Nairobi found such anti-fertility ingredients in the tetanus vaccine administrated as part of a WHO vaccination campaign in Kenya.
Currently, there is evidence that covid vaccines may impact menstruation and possibly pregnancy and neonatal health (if vaccinated during pregnancy), but there is not yet any evidence that covid vaccines permanently impact female (or male) fertility.
Similarly, there is clear evidence that covid vaccines increase the short-term risk of cardiovascular adverse events (see above), but there is not yet solid evidence that they have a long-term impact on cardiovascular health, although this cannot be excluded.
2) Are covid vaccines “vaccines”? Or “gene therapy”? Or both?
Are covid vaccines “vaccines”? Yes, because they induce an antibody immune response.
Bud didn’t the Merriam-Webster dictionary have to change its definition of “vaccine” in January 2021 to include covid vaccines? Yes, but their previous definition was outdated and wrong: it referred to a “preparation of killed microorganisms, living attenuated organisms, or living fully virulent organisms”, which didn’t include toxoid vaccines (like the tetanus vaccine) or protein-based vaccines (like the hepatitis B vaccine) or of course mRNA or DNA vaccines (like some of the covid vaccines).
Are covid mRNA and DNA vaccines “gene therapy”? Yes, mRNA and DNA vaccines have always been regarded as an application of gene therapy, simply because they are based on genetic technology (DNA or mRNA). The European Union even had to suspend some of its GMO regulations to fast-track covid vaccine development and manufacturing.
If covid vaccines are gene therapy, do they alter the human genome? They are not intended to do so. In fact, gene therapy as a whole initially consisted primarily of “gene replacement therapy”, not “gene editing therapy”: a “defective gene” is being replaced by providing the cell with a functioning gene copy as DNA (which then is translated into RNA) or directly as mRNA (which then is translated into protein), without editing the human genome. Only more recent technologies like CRISPR allow to directly edit the human genome.
However, although not intended, both mRNA and DNA vaccines (and the coronavirus itself) could, theoretically and under certain circumstances, insert genetic material into the human genome, although this has not yet been shown to happen in practice.
In conclusion, “covid vaccines” are both vaccines and gene therapy, but are not intended to alter the human genome, and so far haven’t been shown to alter the human genome.


Comments
Post a Comment