The Great COVID Ventilator Death Cover-up
The Great COVID Ventilator Death Cover-up
Tens of thousands of Americans died after being placed on mechanical ventilators in spring 2020. It’s long past time we got real answers as to how many were killed this way.

It’s long been something of a mystery why there have been no major studies on how many COVID patients were killed by mechanical ventilators in spring 2020. Early data from China had suggested that ventilators would need to be used widely in the treatment of COVID patients, and this led to a major rush to procure ventilators on the part of politicians and hospital systems all over the world.
A small sample of the hundreds of headlines from that period features ones such as: “Cuomo refutes Trump, insists NY needs up to 40,000 ventilators,” “NY may need 24,000 more ventilators to fight COVID-19. Here’s how it could get them,” “Which coronavirus patients will get life-saving ventilators? Guidelines show how hospitals in NYC, US will decide,” “Amid Ongoing COVID-19 Pandemic, Governor Cuomo Announces 1,000 Ventilators Donated to New York State,” “A New York hospital is treating two patients on a device intended for one.”
However, it soon became clear that ventilators were being vastly overused, and the medical community gradually ceased this practice of mass intubation. Dr. Cameron Kyle-Sidell acted as an early whistleblower, sounding the alarm in a widely-shared video:
We are operating under a medical paradigm that is untrue… I fear that this misguided treatment will lead to a tremendous amount of harm to a great number of people in a very short time… This method being widely adopted at this very moment at every hospital in the country…is actually doing more harm than good.
In interviews with major media outlets, several practitioners later disclosed that patients had often been put on ventilators not for their own benefit, but in order to stop the virus from spreading. As one doctor later told the Wall Street Journal:
We were intubating sick patients very early. Not for the patients’ benefit, but in order to control the epidemic and to save other patients. That felt awful.
As another doctor told Time Magazine:
He says some doctors are intubating early because they fear that less-intensive forms of ventilation, like high-flow nasal oxygen, can aerosolize a virus, putting health care workers at risk of getting sick. ‘This is more theoretical fear than a real fear,’ Hill says, since there’s not strong evidence that COVID-19 spreads this way.
As Dr. Rich McCormick told the House COVID Select Subcommittee:
The healthcare professionals…got it wrong. We were going off of old technologies, old assumptions. And I remember we were intubating people that probably shouldn’t have been intubated.
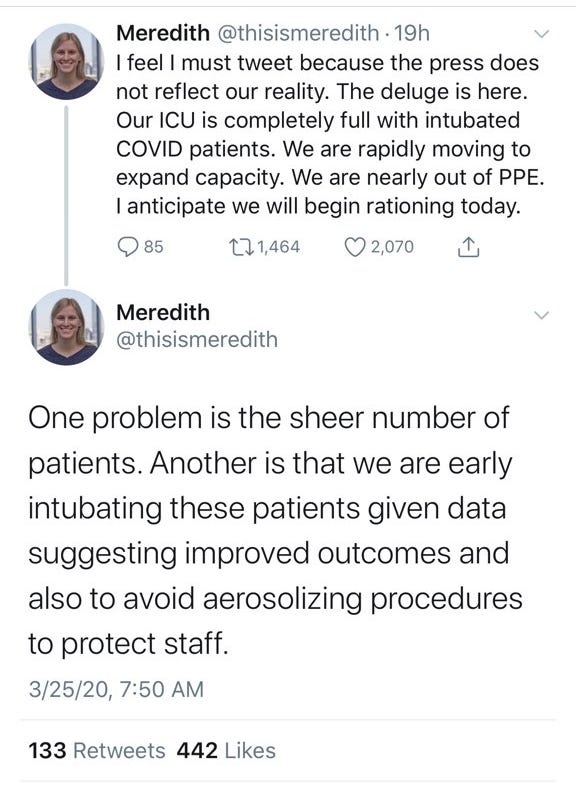
As Meredith Case, an internal medicine resident at NewYork-Presbyterian Medical Center, put it in a series of since-deleted threads, hospitals were “early intubating” patients for “many days if not weeks” in part “to avoid aerosolizing procedures to protect staff,” and several “practice changes lead to more time on the vent.”
One problem is the sheer number of patients. Another is that we are early intubating these patients given data suggesting improved outcomes and also to avoid aerosolizing procedures to protect staff.
1) We are mostly being transferred patients with single organ (i.e. respiratory) failure from other ICUs to offload those units. These patients have been intubated for many days if not weeks. Weaning is slow going
2) The shortages of critical analgesics and sedatives means we are using drugs less well suited to the purpose. Using second (third? fourth?) line meds hampers our ability to quickly wean sedation when oxygenation has improved, further prolonging time on the vent
3) Relatedly, in order to limit the # of times nurses and providers enter the room, we have moved away from our usual plan of IV pushes for analgosedation and toward IV drips because pushes require nurses to enter the room more frequently
4) These practice changes lead to more time on the vent, which in turn means more time to develop complications. Obvious point but important. More HAIs, more deconditioning, more delirium. I have two rising hyperbilirubinemias on my service concerning for acalculous cholecystitis

This practice of extended intubation was apparently consistent with early guidance coming from China. As fanatical mask advocate and free-speech opponent Zeynep Tufekci put it, “Chinese scientists” had advised “many COVID-19 patients need to stay on mechanical ventilators as long as four weeks”:

Some hospitals in New York began engaging in “split-ventilation”—putting patients on ventilators two-at-a-time:
At least one New York hospital has begun putting two patients on a single ventilator machine, an experimental crisis-mode protocol some doctors worry is too risky but others deemed necessary as the coronavirus outbreak strains medical resources.
“Split-ventilation” made intubation even more dangerous than it already was:
Facing a ventilator shortage, doctors are considering using one machine for multiple patients in respiratory failure. But it’s at best a stopgap and can injure the lungs.
As White House Coronavirus Response Coordinator Ashish Jah wrote in NEJM:
[P]atients who are traditionally treated with noninvasive positive-pressure ventilation (NIPPV) for conditions such as chronic obstructive pulmonary disease exacerbations may need to instead be presumptively intubated while awaiting Covid-19 testing results (using NIPPV is contraindicated for patients with Covid-19 because of aerosolization of the virus under positive pressure).
As Dr. John Ioannidis put it in a podcast with Vinay Prasad: “a lot of lives” were lost in spring 2020 in part because of doctors “not knowing how to use mechanical ventilation, just going crazy and intubating people who did not have to be intubated.”
Even Anthony Fauci eventually admitted that having “very very readily put people on mechanical ventilation” may have “caused more harm than good.”
I think the intensive care has improved. We very, very readily would put people on mechanical ventilation, when we found out through clinical experience it might have been better just to make sure we positioned them properly in the prone or supine position and not necessarily to intubate someone so readily, which might have actually caused more harm than good. We learned that as we got more experience.
The New Yorker featured a harrowing account of one early victim’s experience titled The Life and Death of Juan Sanabria, One of New York City’s First Coronavirus Victims describes Juan Sanabria’s final moments of consciousness before he was intubated:
At eight o’clock the next morning, the doctor called Walkiris and asked her to help persuade Sanabria to be intubated. He’d deteriorated overnight, and now needed to be on a respirator. “Am I going to die?” Sanabria asked Walkiris. “No, pápi,” she told him. “They’re going to put you to sleep for a little while, so you can relax your lungs. You’re breathing too fast.” He seemed dazed. “I don’t feel sick,” he said calmly. “Will you be here when I wake up?”
“I’ll see you on the other side,” she replied. “Let them do this.” As the nurses prepared to intubate him, he bragged about how his daughter was a nurse. Just before he went under, he sent Walkiris one last selfie…
The next day, Juan’s blood pressure dropped precipitately. Walkiris’s sister and mother tried to visit him in the hospital, too, but were turned away. They told Walkiris to pray. “I kept telling them, ‘Look at this chart. He doesn’t even have a few days,’ ” Walkiris said. “My family didn’t want to hear it.” He never regained consciousness after being intubated; by the time he died, on March 17th, no one had been able to say goodbye.
Indeed, this practice of mass intubation proved extremely deadly. A study in JAMA later revealed a 97.2% mortality rate among those over age 65 who’d been put on mechanical ventilators. To put this in perspective, patients over age 65 were more than 26 times as likely to survive if they were not placed on mechanical ventilators.
Overall, mortality among COVID patients in New York area hospitals fell by over two-thirds between spring 2020 and summer 2020.
The available evidence has always overwhelmingly indicated that ventilators killed many patients in spring 2020. However, until now, it’s been difficult to argue there was necessarily any kind of cover-up going on. Yes, some patients had been killed by ventilators, but there were, quite simply, not very many people talking about this issue. Rather, the simple explanation for why there had been no serious assessments of the number of patients killed by ventilators was that so few people were asking for them.
But this all changed dramatically in just the last couple weeks as the ventilator issue came roaring back into mainstream discourse. Most notably, a viral thread by Dr. Craig Spencer brought the ventilator question back into the spotlight.
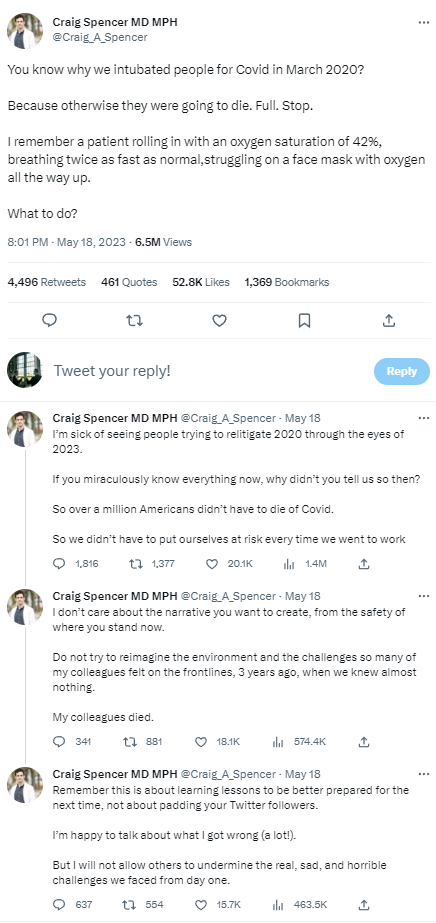
There’s a lot wrong here. First, Spencer’s initial assertion that all the patients who were put on ventilators were going to die anyway directly contradicts his subsequent, defensive assertion that it’s unfair to “relitigate 2020” because we can’t relate to those kinds of high-stress frontline decisions. If all those patients had actually been bound to die anyway, then there wouldn’t be any mistakes to “relitigate.” And, if this policy of mass intubation was working so well that all the patients who died on ventilators would have died anyway, then there would have been no reason for the medical community to have ever stopped doing it.
That this self-contradictory thread has so many “likes” is somewhat troubling—a sign of just how widespread complicity is in propping up the logically-incoherent official COVID narrative. But the fact that so many people have gotten behind this ludicrous narrative actually presents a promising opportunity. For the first time, we now have something close to an official explanation of why there haven’t been any studies on how many patients were killed by ventilators.
In short, the establishment is trying to argue that while ventilators were overused in spring 2020, doing more harm than good—and the vast majority of patients placed on ventilators died—the ventilators themselves did not kill anyone. An astonishing argument, even by the abysmal standards of the COVID era.
But, since everyone supporting this narrative is arguing that there were no ventilator deaths in spring 2020, all we have to do is prove there were a significant number of ventilator deaths and what’s left of the establishment’s credibility on the initial months of COVID falls apart.
In addition to the anecdotal evidence discussed above, several unsettling data points have long strongly suggested that there weren’t just some ventilator deaths in spring 2020, but rather a pretty frightening number of them.
As a preliminary matter, the data bears out that ventilators were used very readily in spring 2020, especially in the greater New York area, and that ventilator use was sharply curtailed after that period. The CDC reports that 18,679 patients died with COVID in New York City hospitals throughout spring 2020. And, according to the sample in JAMA, just over half of those who died with COVID in NYC hospitals were put on ventilators. Accordingly, around 10,000 patients died with COVID in NYC hospitals after being put on ventilators in spring 2020.


As I’ve previously written, the percentage increase in excess deaths in the greater New York area in spring 2020 vastly outstrips the percentage increase even in other cities with similar climate and social and economic demographics, indicating an unbelievable number of deaths owing to iatrogenesis, ventilators and strict lockdowns in the greater New York area in spring 2020.

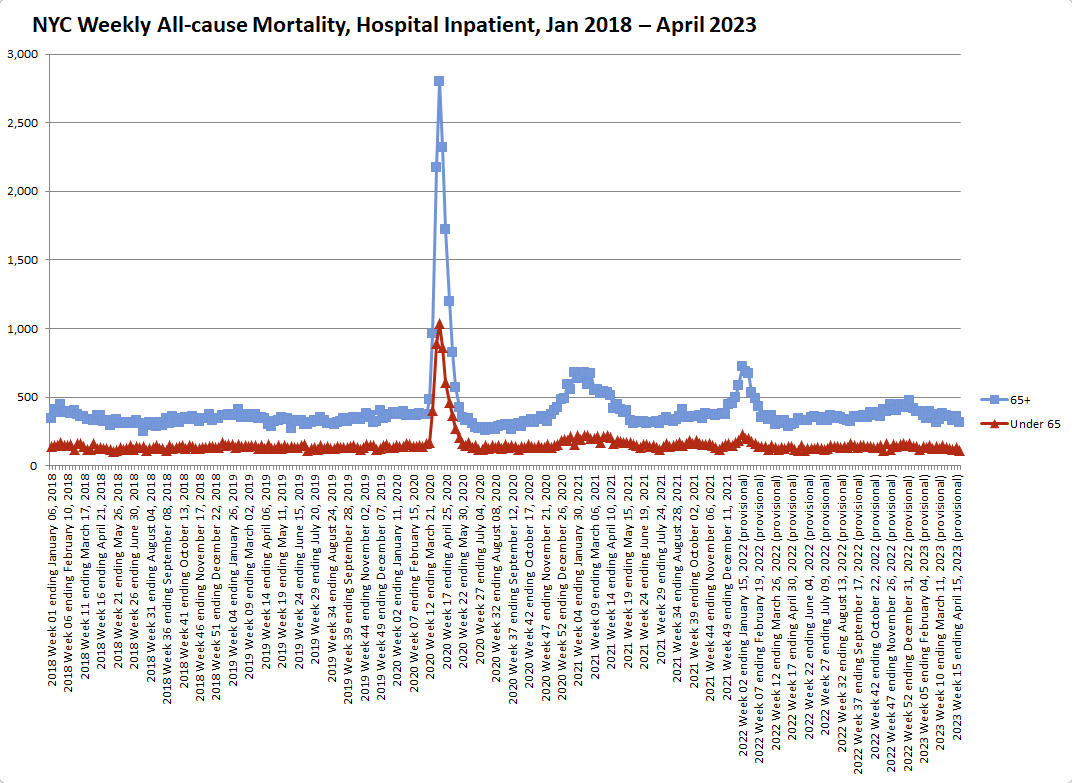
Additionally, as Jessica Hockett has documented in meticulous detail through multiple methods, New York City experienced a sharp, breathtaking mortality event just after its lockdown and response to COVID began, which was unlike that experienced anywhere else or at any other time. Given its singularity, this horrifying mortality event, quite simply, cannot be attributed to natural causes.
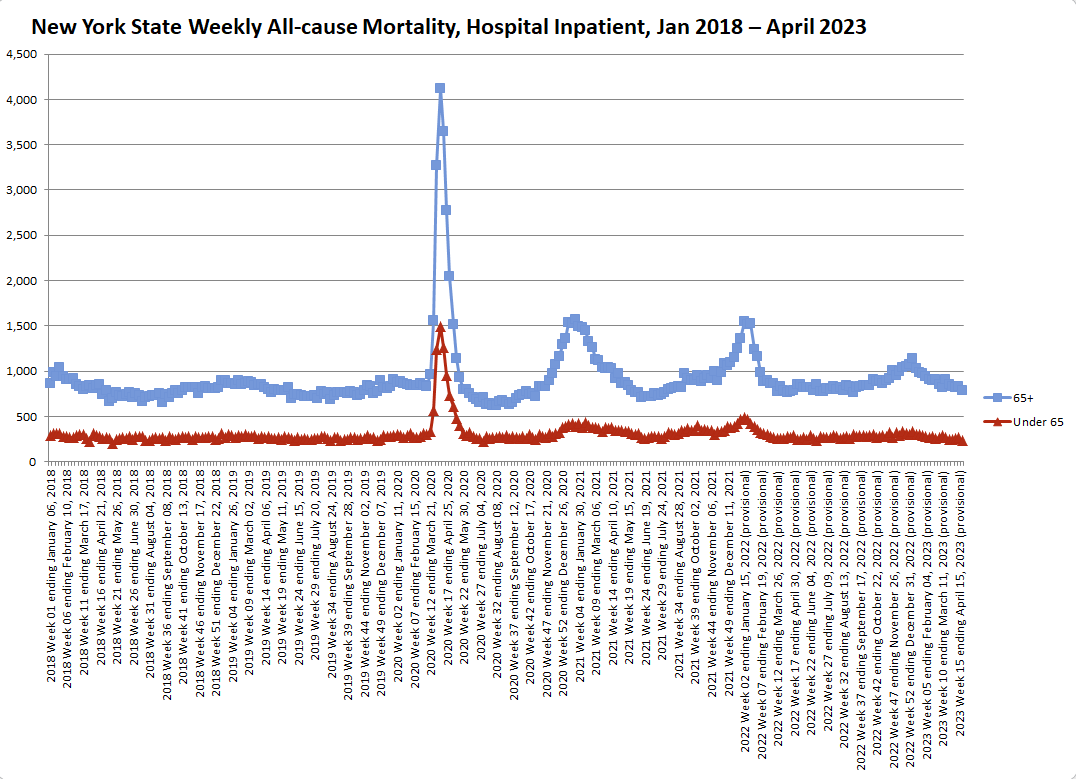
Jumping off Hockett’s work, below is a chart of weekly all-cause hospital inpatient mortality from January 2018 through April 2023, split between patients ages 65+ (blue line) and patients under 65 (red line). This spike in inpatient hospital mortality in New York City in spring 2020, especially among young people, is unparalleled in any other time period, even as COVID deaths supposedly began to climb again in 2021.
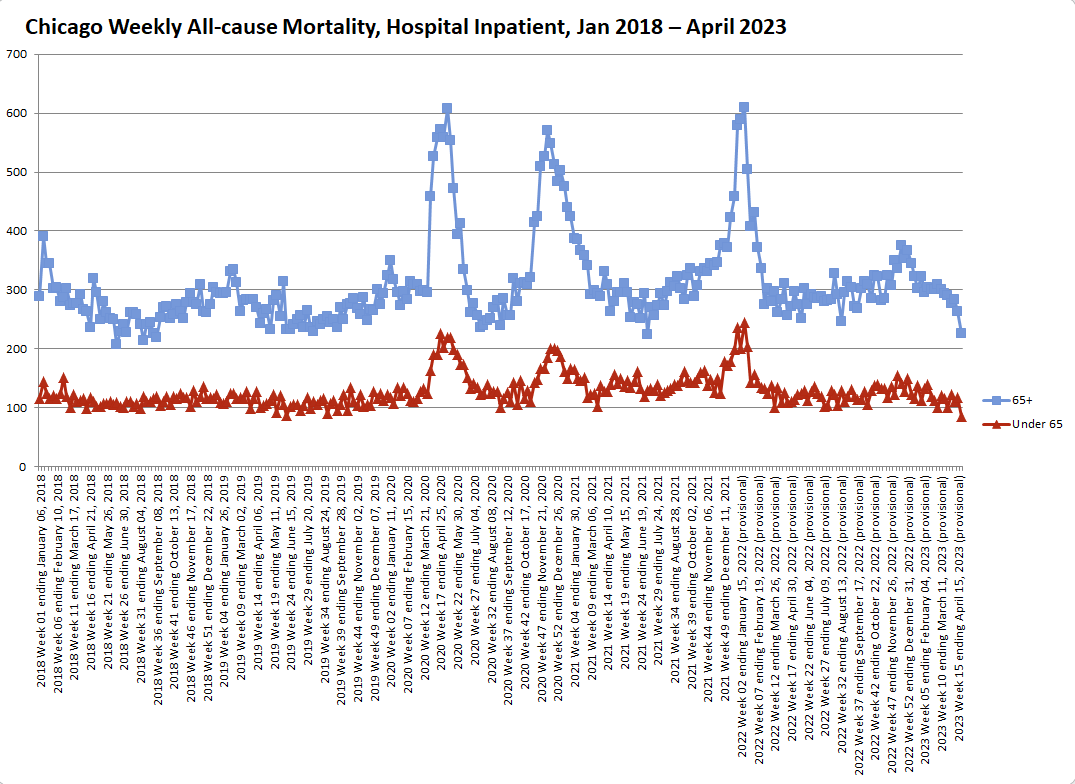
For comparison, below, I’ve produced this same chart for each of America’s largest metropolitan areas: Chicago, Dallas, Houston, Los Angeles, and Washington, DC. (All data is from “CDC Wonder Provisional Mortality Statistics, 2018 through Last Month.” Data is collected at the county level; only data from counties typically considered part of each of these cities has been included.)
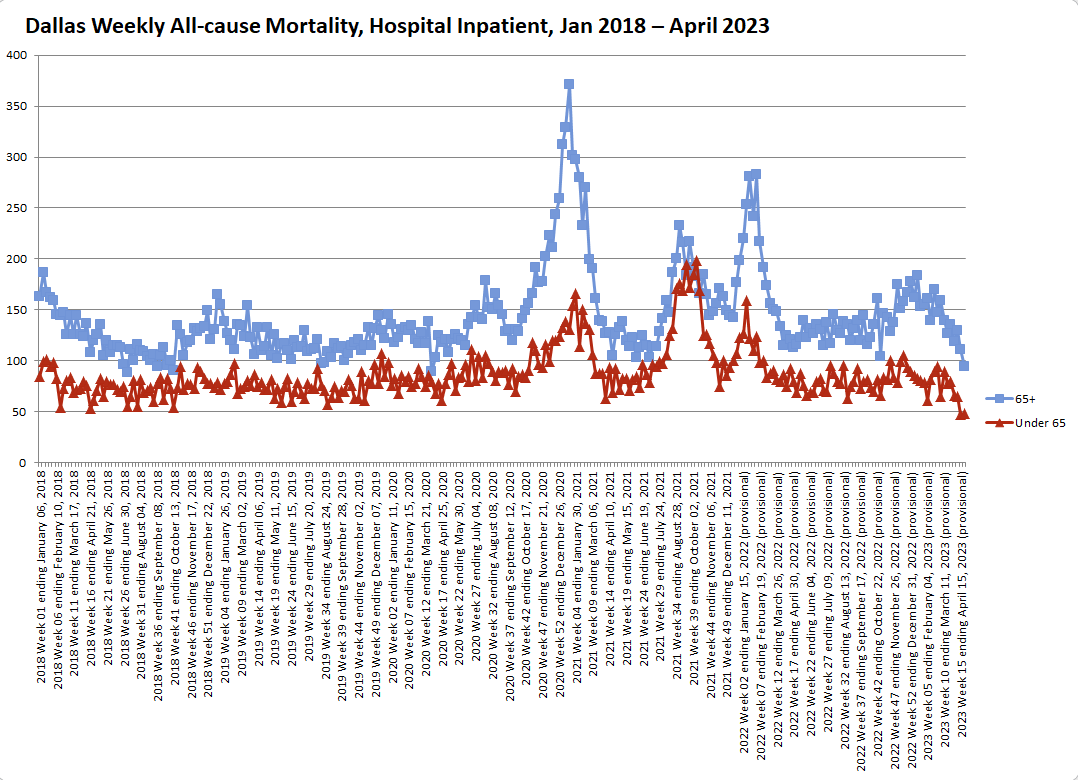
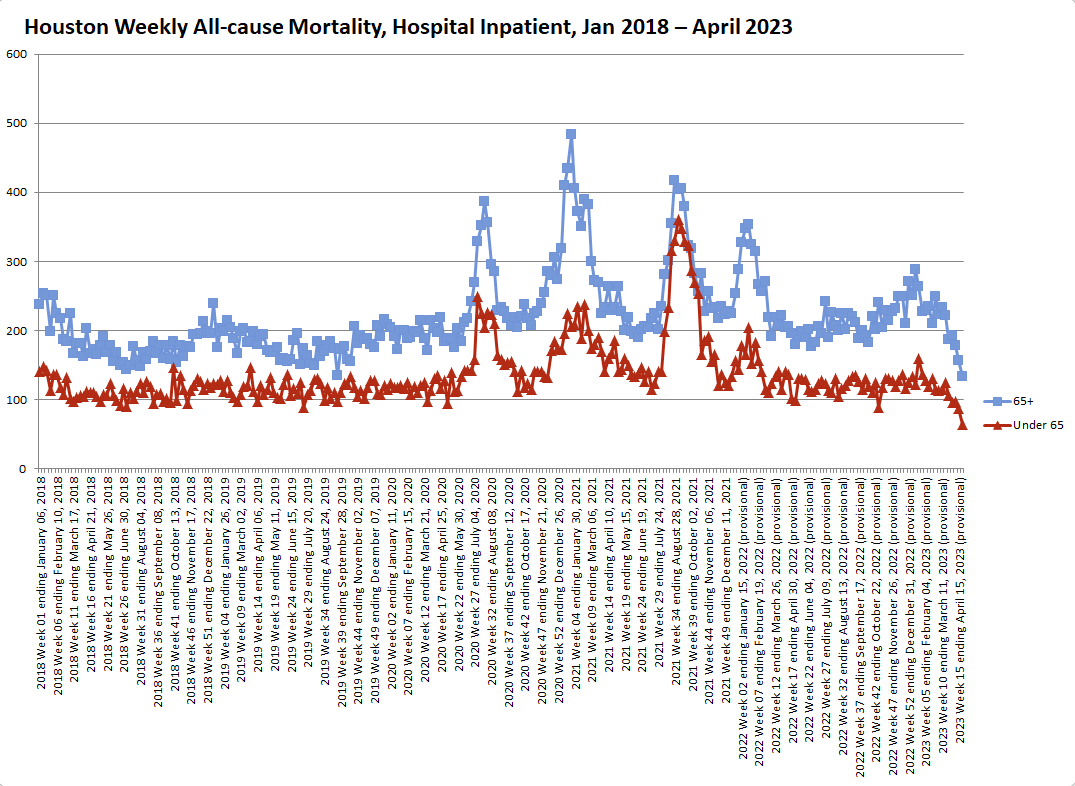
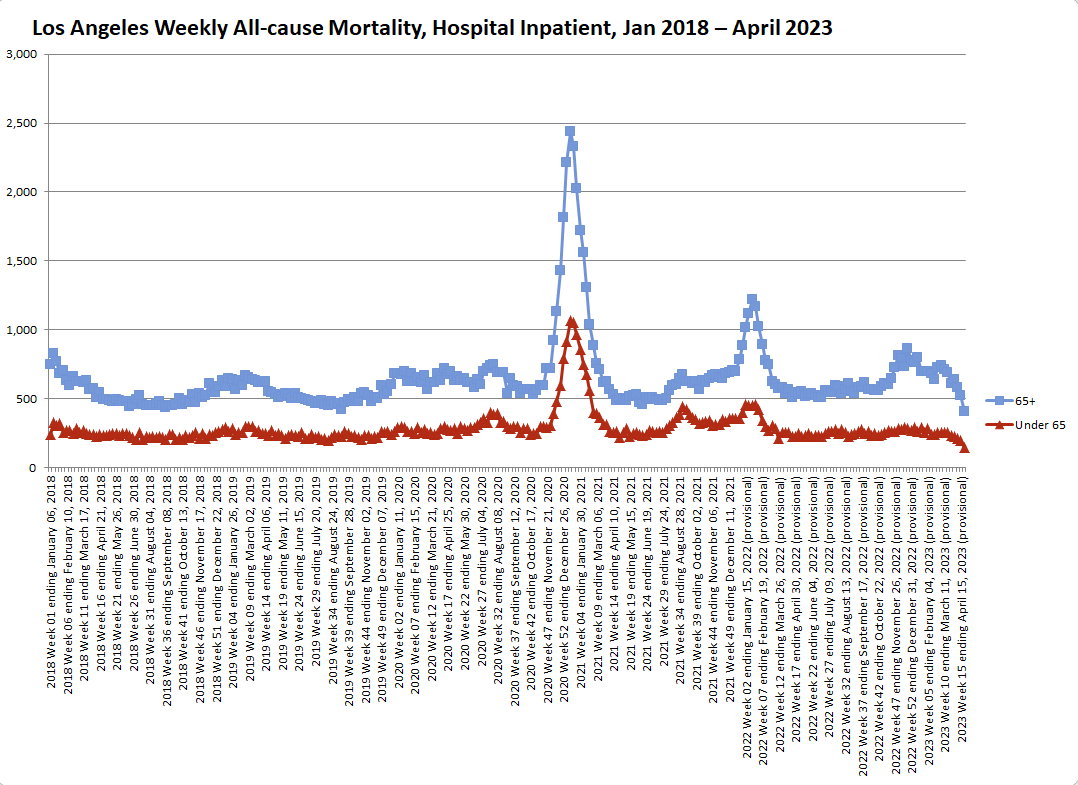
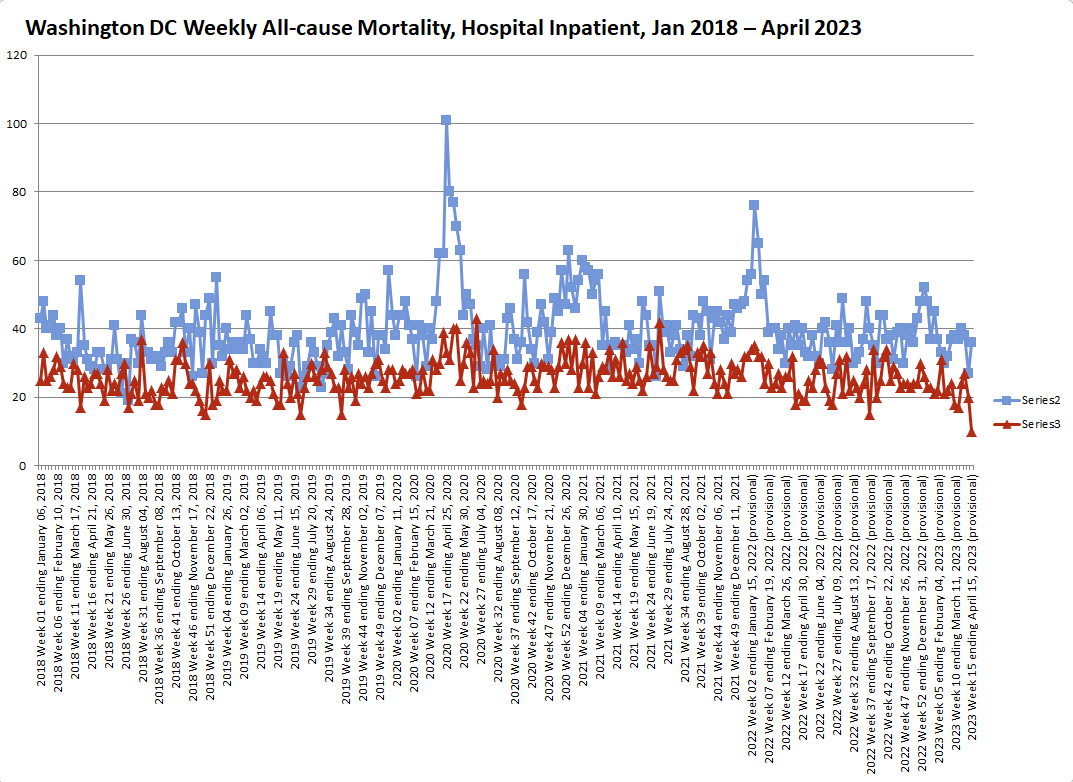
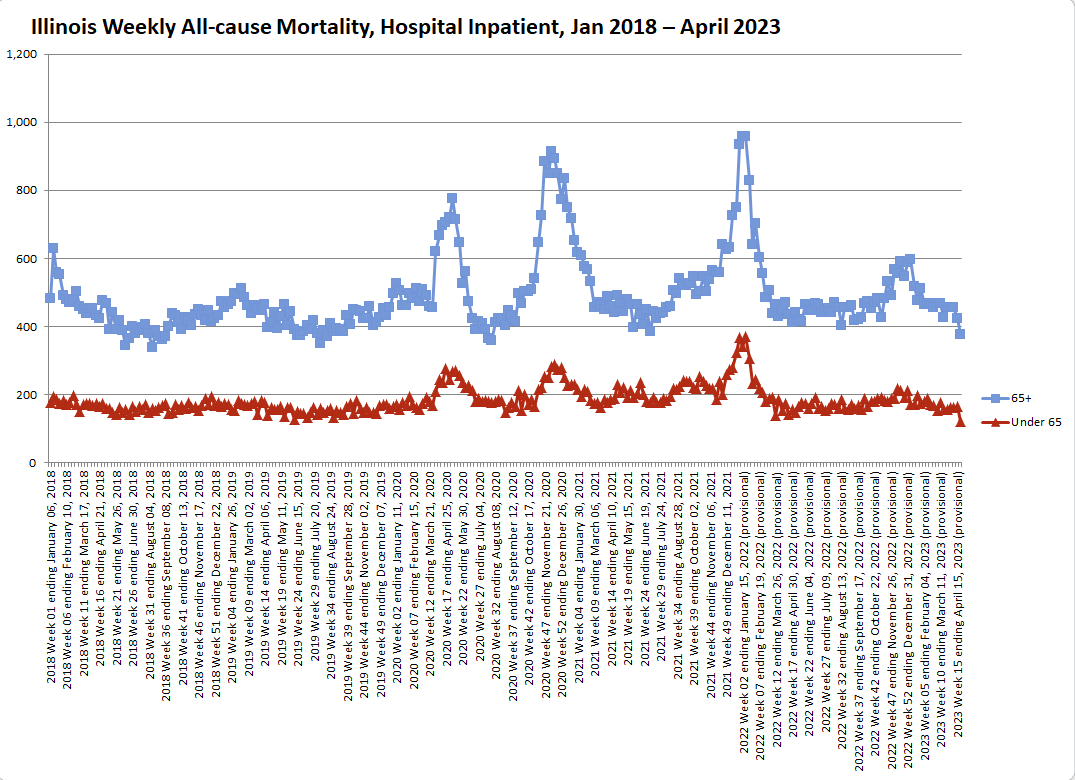
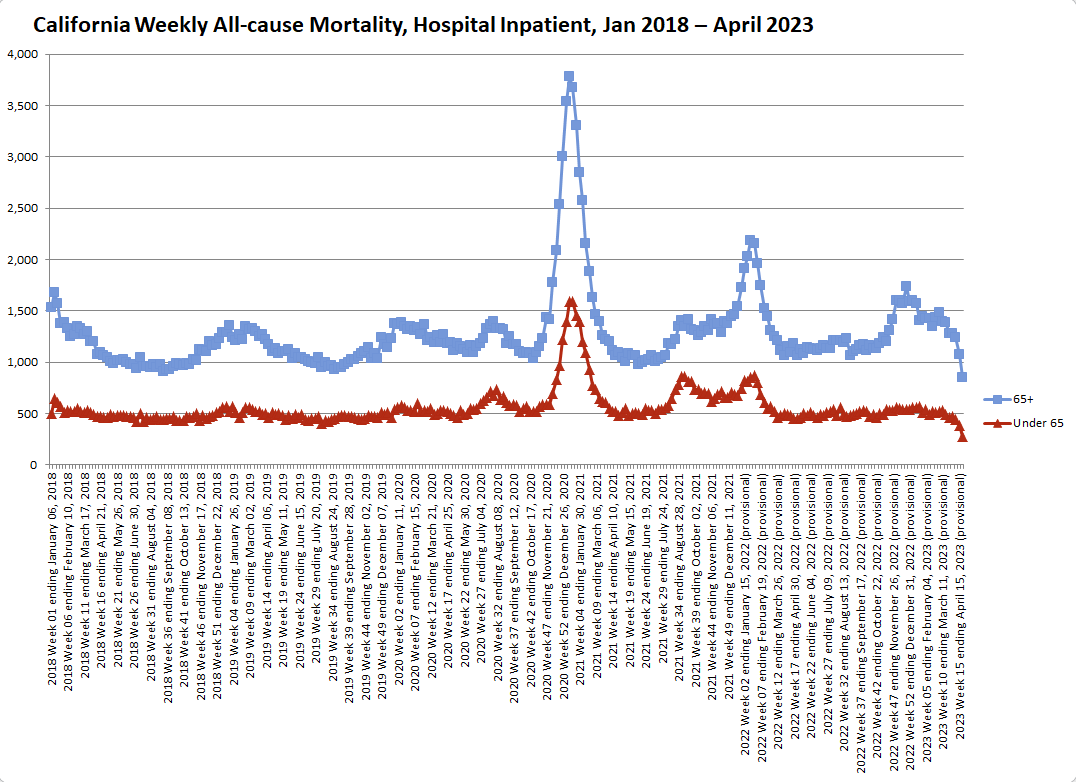
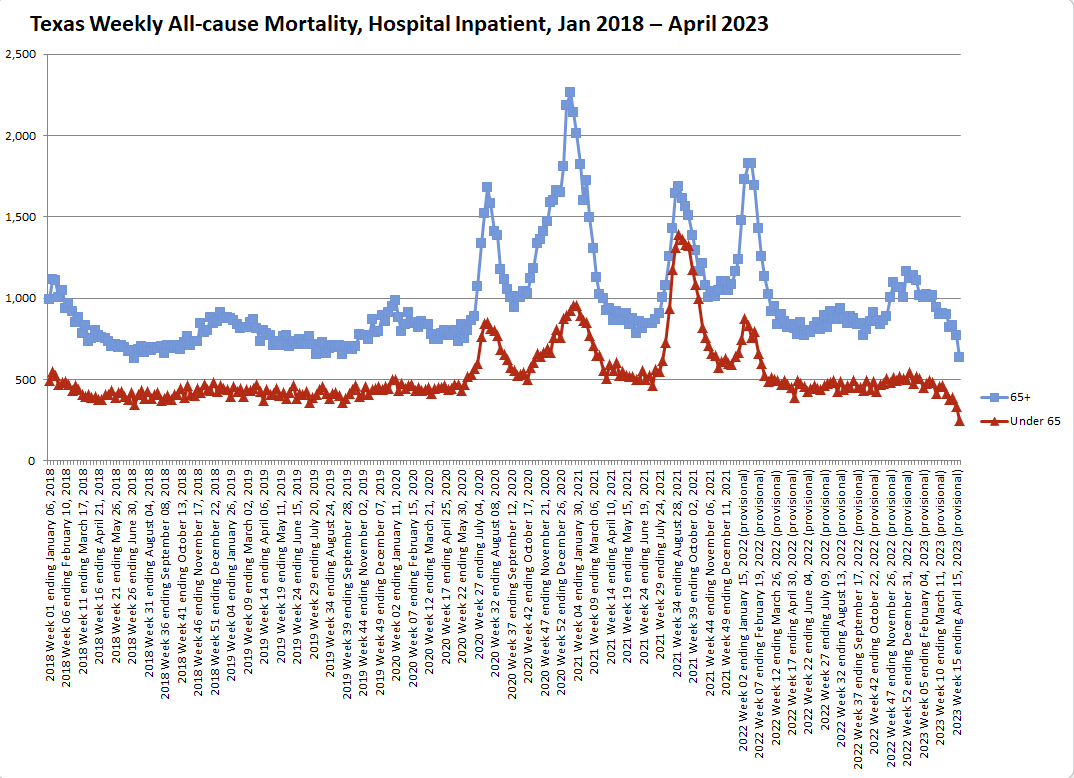
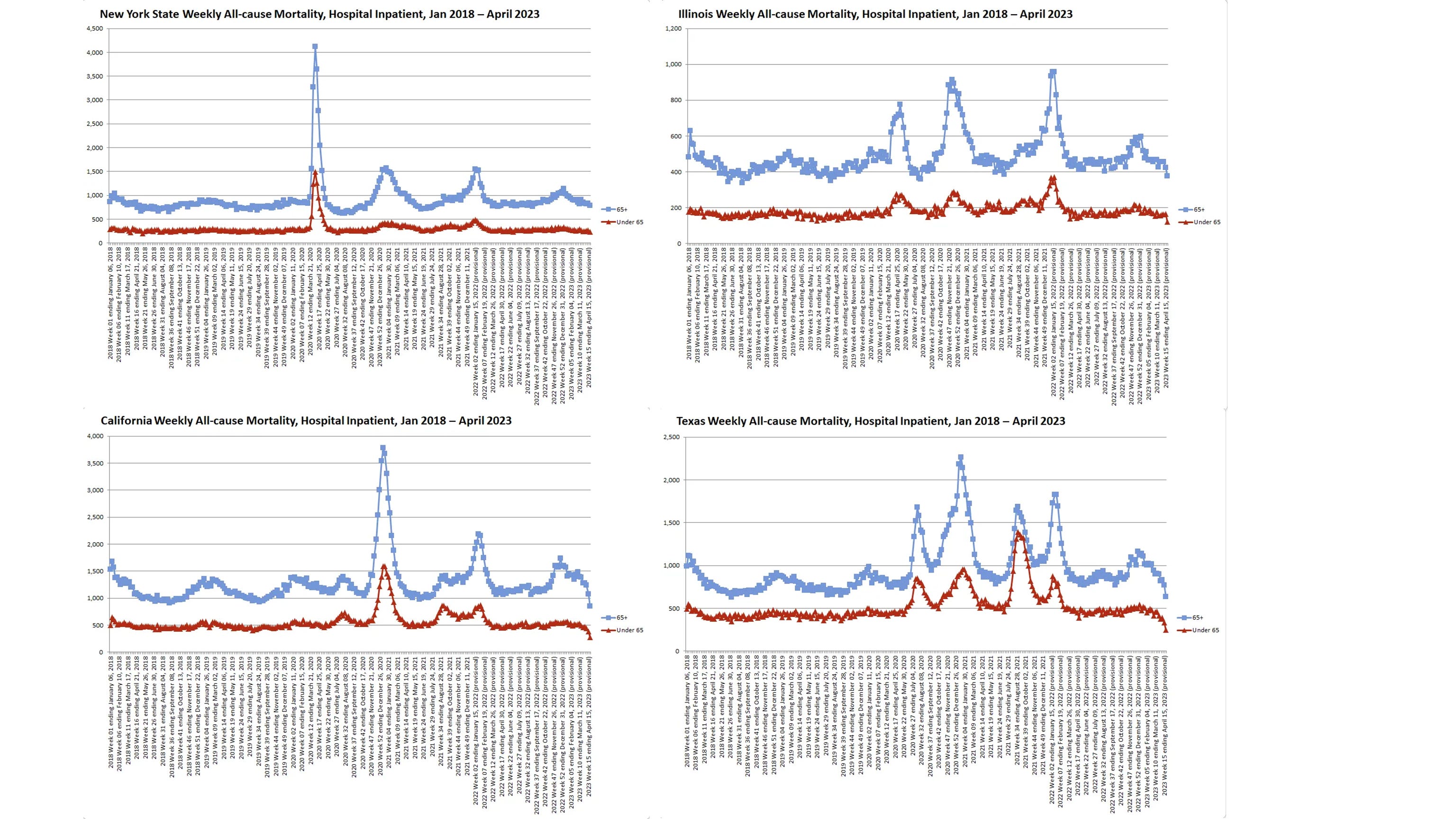
And here is the same chart for each at the state level:
Here are each of these charts juxtaposed in high-resolution images for purposes of side-by-side comparison. (You’ll need to right click and select “Open image in new tab” to zoom in.)
City level data:
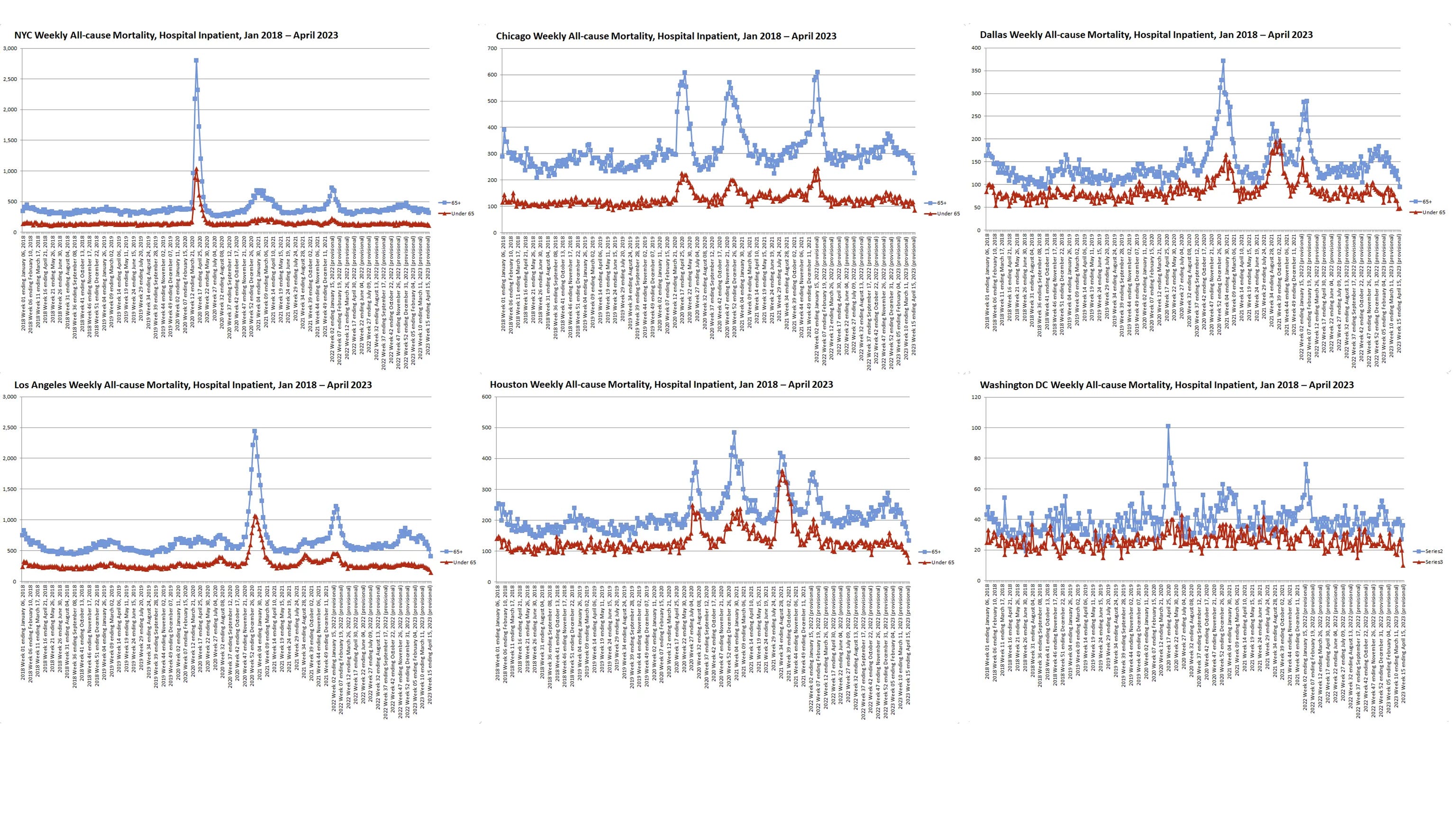
State level data:
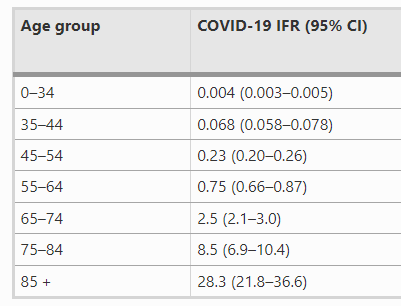
A couple of points on these charts. First, while the spike in mortality in the NYC area in spring 2020, especially among young people, is without parallel, it’s not the only one we see. These spikes in mortality among young people are conspicuous because it’s long been known that COVID’s infection fatality rate (IFR) is extremely skewed toward the elderly. This, for example, is the most widely-cited data on COVID’s IFR by age:
Thus, these spikes in mortality among young people cannot be attributed to COVID. Most notably, a significant spike in mortality appears among all age groups in California at the end of 2020—albeit not of the same magnitude as that in New York in spring 2020. One possibility is that, while the use of ventilators was generally scaled back, hospitals in California may have still been engaging in broad intubation or other iatrogenic practices by the end of 2020. Another possibility is that this spike in deaths in California was a byproduct of lockdowns and the fear that accompanied them; while one might expect lockdown deaths to be more normalized over time, increases in respiratory virus deaths tended to be accompanied by more restrictions, more fear, and thus more lockdown deaths. Even more strangely, Texas experienced a surge in deaths among young people in summer 2021 that was not accompanied by a corresponding increase in mortality among the elderly; this, frankly, may have had nothing to do with COVID.
That said, the fact remains that the New York area experienced a uniquely sharp, awful mortality event in spring 2020 which is not adequately explained by any of these other factors. And doctors were under significant pressure to put patients on ventilators in spring 2020, even if it was merely unconscious; politicians had purchased tens of thousands of ventilators at exorbitant prices, and hospitals did receive more funding if patients were placed on ventilators. Coupled with the above anecdotes about patients being placed on ventilators for extended periods to protect staff—and the fact that over 10,000 patients in New York City died after being intubated—it’s clear that a horrifying number of patients were likely killed by mechanical ventilators.
Yet astonishingly, despite all these facts, the establishment is arguing that no patients were killed by ventilators in spring 2020.
This, to me, is the kind of implausible, overly-defensive argument one makes when they’re panicked. Across America, tens of thousands of patients were placed on ventilators in spring 2020; given the vast majority of those patients died, it simply begs credulity that none of them were killed by ventilators. When a deadly procedure is applied to tens of thousands of patients, even a baseline level of human error would imply that the procedure was applied to at least some fraction of those patients by mistake.
The establishment has responded with subsequent studies claiming to show that “early intubation” actually reduced the time patients spent on ventilators, and thus didn’t kill any of them. But this is a straw-man argument. As the above anecdotes make clear, the issue isn’t whether patients were intubated “early” or “late” relative to any symptoms they might have shown—the issue is whether patients were placed on ventilators who should have never been on them to begin with, or otherwise kept on them too long.
Even more strangely, most of the attorneys with whom I’ve discussed the ventilator issue agree that—outrageous as it may be—there’s actually little litigation risk for the medical establishment because of the perceived global emergency in spring 2020. Regardless of how much harm was done, it’s simply too difficult to prove that the procedure violated the emergency standard of care given the information coming from China at the time.
This also explains why no one has yet taken the hospitals to court on the ventilator issue. If anyone wants to fight the establishment for real answers as to how many patients were killed by ventilators, the time and money for this cause will have to come on a charitable basis. Doubtless, the medical establishment’s high-priced lawyers are well aware of this fact—and this, too, leads me to believe that the real number of patients killed by ventilators must be frighteningly high; even absent any real litigation risk, the embarrassment alone is leading to this broad cover-up.
Nonetheless, the situation is morally inexcusable. It’s imperative that we get the truth of how these patients died, not only so we can put together what really happened in spring 2020, but also because it’s the least we can do to honor the deceased.
Speculating as to how it got to this point, I suspect the medical establishment didn’t want to disclose the number of ventilator deaths in spring 2020 in part out of embarrassment and in part because they thought it might undermine the official narrative and be used by opponents of COVID mandates (remember, we were the “bad guys” at the time). Now that the official COVID narrative has turned into something of a catastrophe and they’ve been sitting on this massive, morally-indefensible cover-up for so long, they just keep digging themselves deeper.
Given all the clumsy, self-contradictory arguments coming from the medical establishment, you’ve probably gathered that, unlike some of the characters I’ve sketched in my work, these are not sophisticated crooks. Rather, these are ordinary people who got into this profession because they wanted to help and now can’t seem to face what really happened. As I detailed in Snake Oil, it’s the hallmark of a great dictator to be able to bring out the evil even in ordinary people—and some men are uncannily good at what they do.


Comments
Post a Comment