boosters associated with higher death rates
boosters associated with higher death rates
the english data is (unfortunately) tracking as predicted
this appears to be some good work by OS who seems to be coming towards some of the same conclusions i have. they seem to be making a real effort to find and establish relationships and rule out effects and so i’d like to provide some of my own thoughts on what they are seeing.
note: 0.51 is a VERY high R2 in a system this noisy and multi-factorial. obviously, correlation is not causality, but this is not a level of correlation one would dismiss without seeking explanation either.

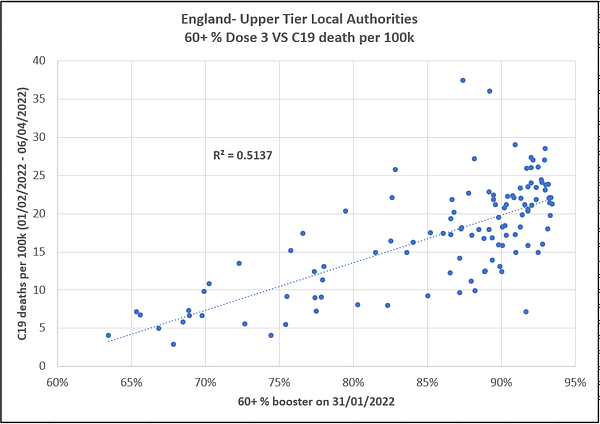
this relationship is one we’re seen all through the US as well. the extremely high vaxx rate states have had more covid hospitalization than in the prior year despite a less virulent variant and given that we saw such rises in the over 70 demographic that was 95%+ double vaxxed in such places, the idea that it was some sort of much higher rate in the non-vaxxed is pretty much mathematically impossible.
we’re seeing the same in israel.
this is an area i have covered in some detail.

so, the trends that OS is pointing out appears to be widespread. they went on to seek to eliminate cross cofounds, which seems wise as these has often been and issue and simpson’s paradoxes abound in this data:
what’s fascinating is the chart on the right: deaths per 100k did not correlate to the % of the county population that is over 60. that is a deeply surprising result given all we know about covid and finds uneasy confluence with the persistently high all cause mortality in the 25-45 segments in many countries.
(OS, should you chance to read this and have some time, that would be a very interesting analysis to perform on the same counties during a pre-vaccination period, say late 2020, to see if this is a relationship that has changed over time as that could provide some useful insight)

this did not correlate to deprivation either.

so we are left with a strong correlation of boosting to deaths. we’re also left with lots of claims and even some apparent data that boosting reduces severity and death. the danes have provided data such as this which appear very interesting and stand in some contrast to the UK data in many regards.
i believe i can explain the variance.

let’s look first at “cases” aka “positive tests.” admittedly, this is a terrible metric with little clinical significance given the widespread testing of asymptomatics using high Ct PCR, but it’s what we have.
the danish data shows no difference among unvaxxed, vaxxed, and boosted. this right there should give real pause on any ideas of vaccine efficacy but could also simply be the well known issues with mRNA training immune response not to pathogen but to the effects of pathogen in the cells and thus being an inherently non-sterilizing modality.
it also shows a consistent lack of difference between the double jabbed and the unjabbed in all measures of severe outcome (hospital, ICU, deaths). it does, however, claim strong efficacy from boosters.
this roughly aligns with UK data (who are no longer reporting double jabs) but with the one large variance that the double jabbed in the UK are now 3-4X as likely to contract covid “cases” as the unvaxxed and this trend keeps widening. (the under 18’s a likely a simpson’s paradox)
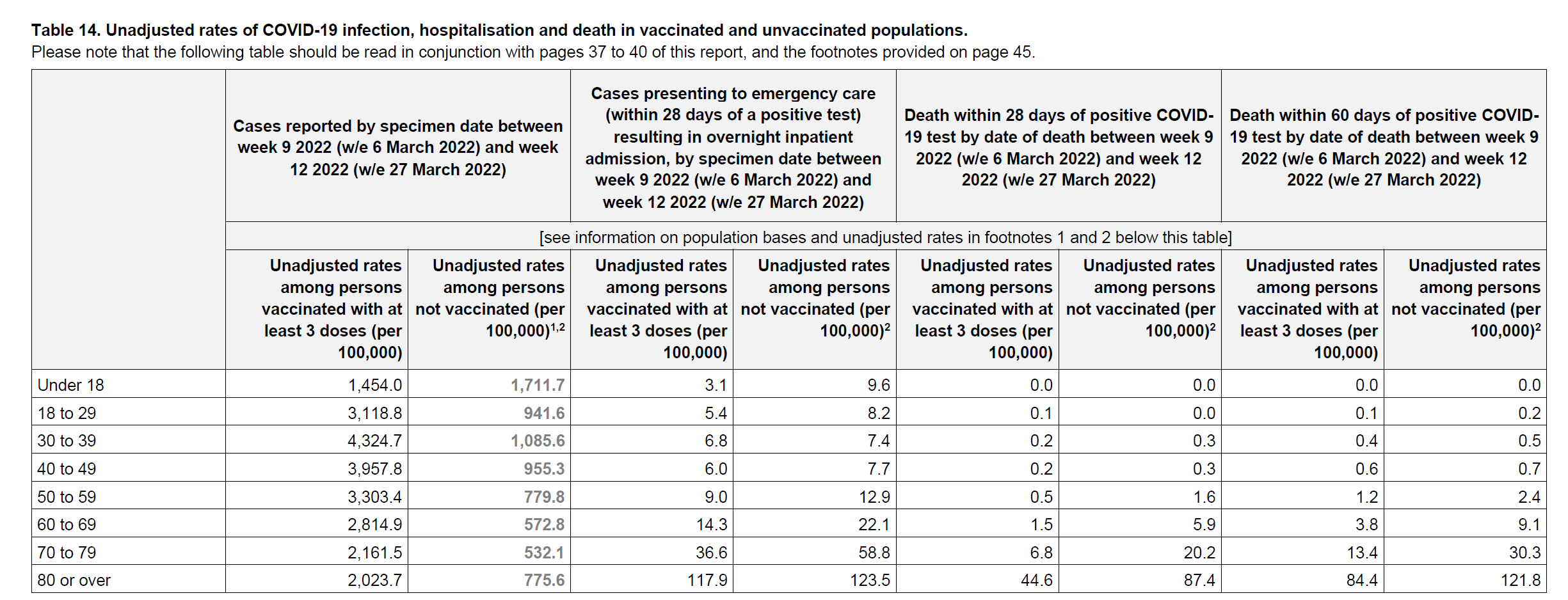
but the UK as well is showing boosters are a mitigating severe outcomes and deaths. but, as we saw above, this is not showing up in the aggregate data. so something is amiss and (as i can see many of you hopping up and down) i’ll get to the point:
it’s because boosters are not working. their efficacy is mostly being conjured into apparent existence through the use of definitions that rig the bayseian analysis.
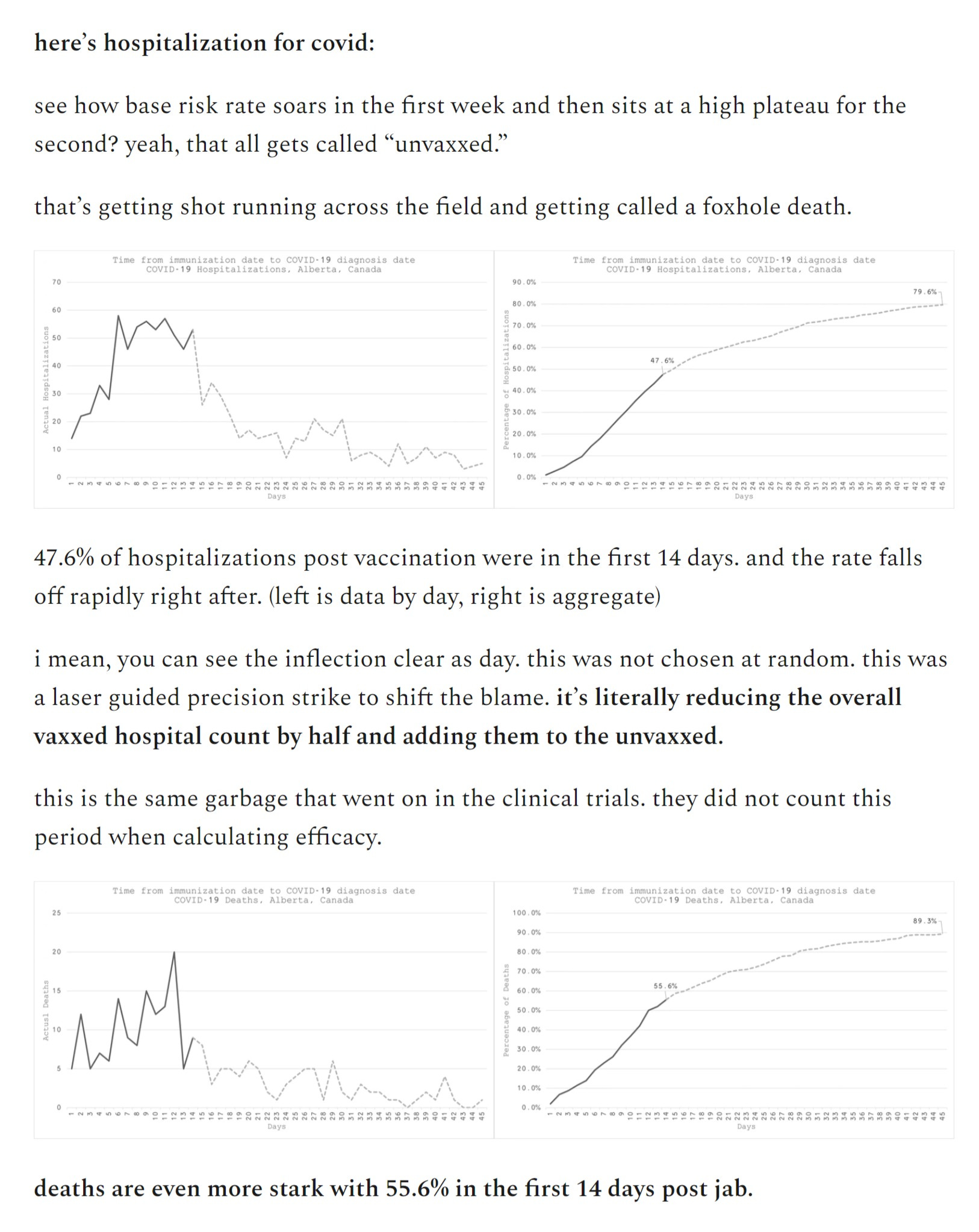
this is another topic on which i’ve written a fair bit. the process is simple:
covid vaccines exhibit well documented immuno suppressive properties in the ~2 weeks post administration
but one is only counted as “vaxxed” at whatever dose is being assessed + 14 days
so this high risk period is not only ignored, but often actually lumped into the prior cohort’s aggregate outcomes.
thus, you get your booster, you get sick 4 days later, but that sickness is either ignored or counted as a case in double vaxxed. this was used to astonishing effect early on to make vaccine driven covid surges look like they were all in the unvaxxed.
this set of definitional legerdemain was 100% deliberate. folks like pfizer are among the best in the world at trial design. they do not make mistakes, they make choices and if i can spot this instantly, so can they. as you’ll see, that 2 week timing is well optimized to maximize apparent effect.
but this jig starts to work against itself as this issue always accrues to the penultimate grouping. boosters shift this set of bad outcomes to the double vaxxed. (many have posited that this is why the UK will no longer report them)
clearly, this is no way to count. it’s a rigged game that is outright ascribing getting hit by a car trying to cross the road to having stayed on the sidewalk because only those who successfully cross the road safely get counted as having tried. more HERE
and as can be seen HERE the effects on reported efficacy are massive. this could easily be the whole ball game.
excerpt:
to my mind, what has happened is simple: we used a set of leaky vaccines that failed to provide sterilizing immunity and that ultimately accentuated spread.
we overstated their efficacy on severity by wide margins (or possibly conjured it completely) by using bayesian datacrime.
these vaccines generated strong antigenic fixation teaching one antibody response that immune systems are exhibiting to preferentially and preventing them from adapting to changing pathogens. (OAS/hoskins effect)
this potent combination has created an ideal evolutionary gradient for vaccine accelerated OAS escape variants to which the large vaccinated cohort cannot adapt well.
they are selecting with unerring precision for the variants (like omicron) that not only evade but are outright advantaged by them.
the data from israel on this is deeply concerning. it looked like perhaps vaccines were working (or at least that herd immunity was taking hold, it’s difficult to separate the two), but then omi hit and everything changed. (full take HERE)
one might be tempted to blame a variant here, but i think we can mostly rule that out.
this is a variant/vaccine interaction.
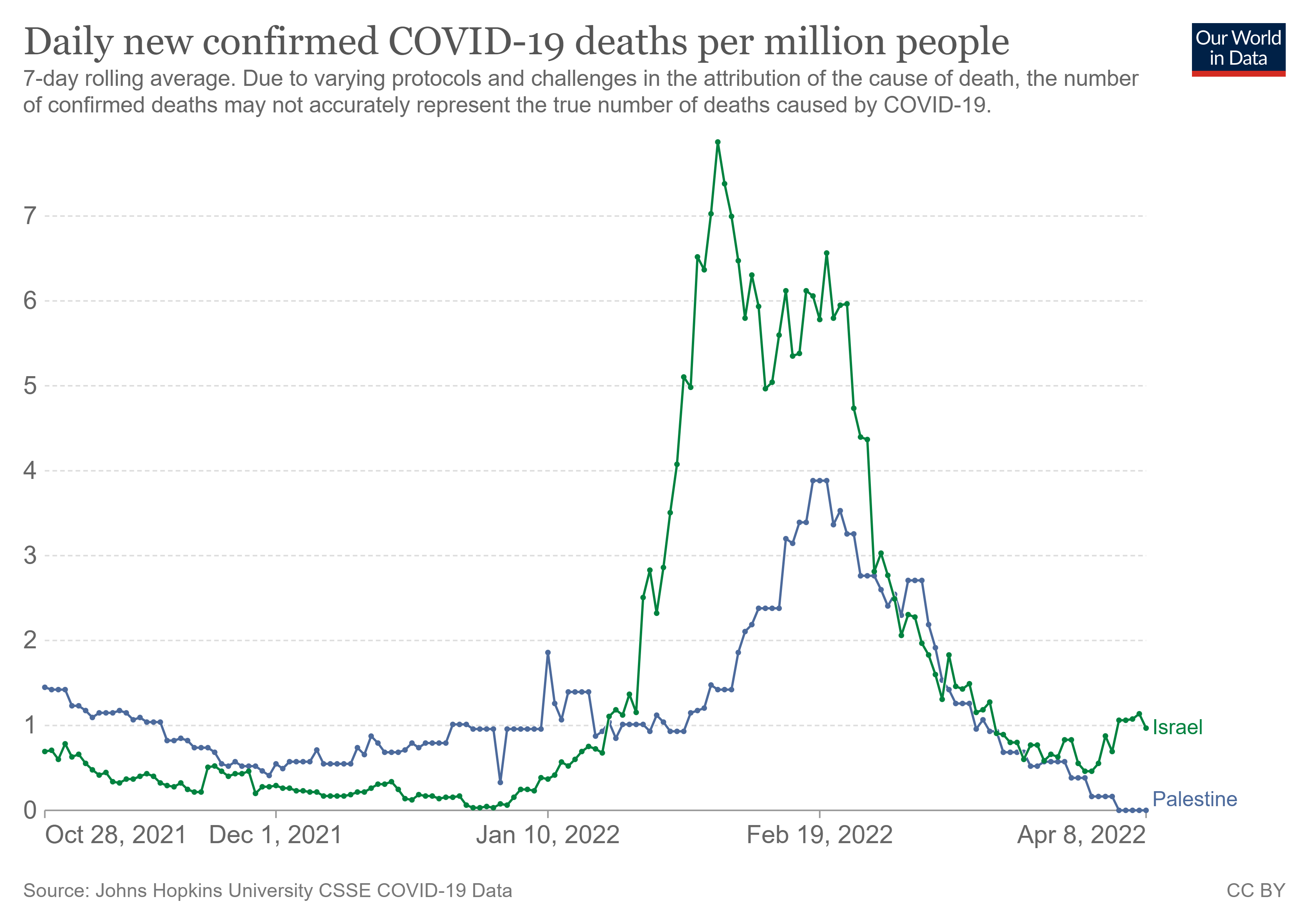
it did not have the same effect in low vaxx palestine despite the two having been so remarkably similar (near identical) throughout. (until now)
the change was sudden and the curve bent the wrong way for vaccines to be working.
also note the odd, out of season uptick in israeli deaths beginning to take hold.
the frightening part if this is what it looks like (admittedly a hypothesis but one that’s gathering an awful lot of confirmation) then this is likely not over. it’s just getting started.
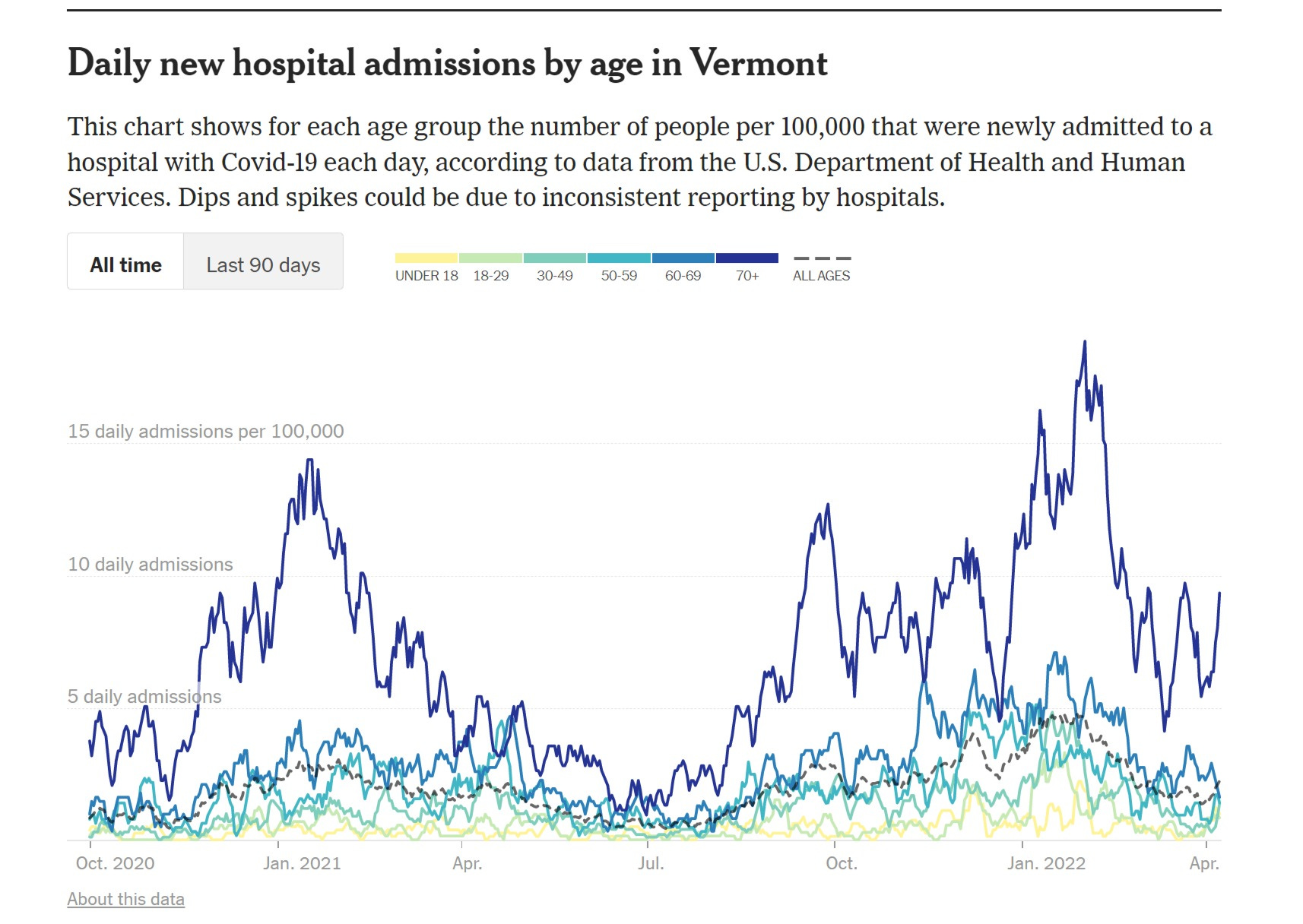
take a careful look at the vermont hospital data above. its’ not only elevated from last year, but currently ticking back up during a seasonal period that ought to show decline. (similar to israel)
this is an unexpected result and one that is counter to booster efficacy (but consistent with herd level antigenic fixation). this is reason for concern.
widespread and identical immunogenic fixation is the opposite of herd immunity. it’s perpetual herd vulnerability and evo-selection for an endless stream of variants that can take advantage of it.
your immune system becomes a one trick pony and so the virus evolves to trick the pony. this does not go well for the pony rider.
i really, really hope to be wrong about this because if this hypothesis is correct (and let’s be clear here, it’s a hypothesis and i’m not sure anything like this has ever happened in human history before so we’re a bit off the edge of the map and into some strange waters) then the vaccines are going to have opened up the inoculated for a life of high susceptibility to covid and will outright breed the variants that will keep making that worse.
that would represent the greatest public health policy disaster in history.
to the extent we see case rates relative to the unvaxxed keep spiking higher and higher and the triple vaxxed get slated by the quad vaxxed etc while overall counts start to spiral up, especially out of season and by breaking with prior age distributions, we’ll see confirmation.
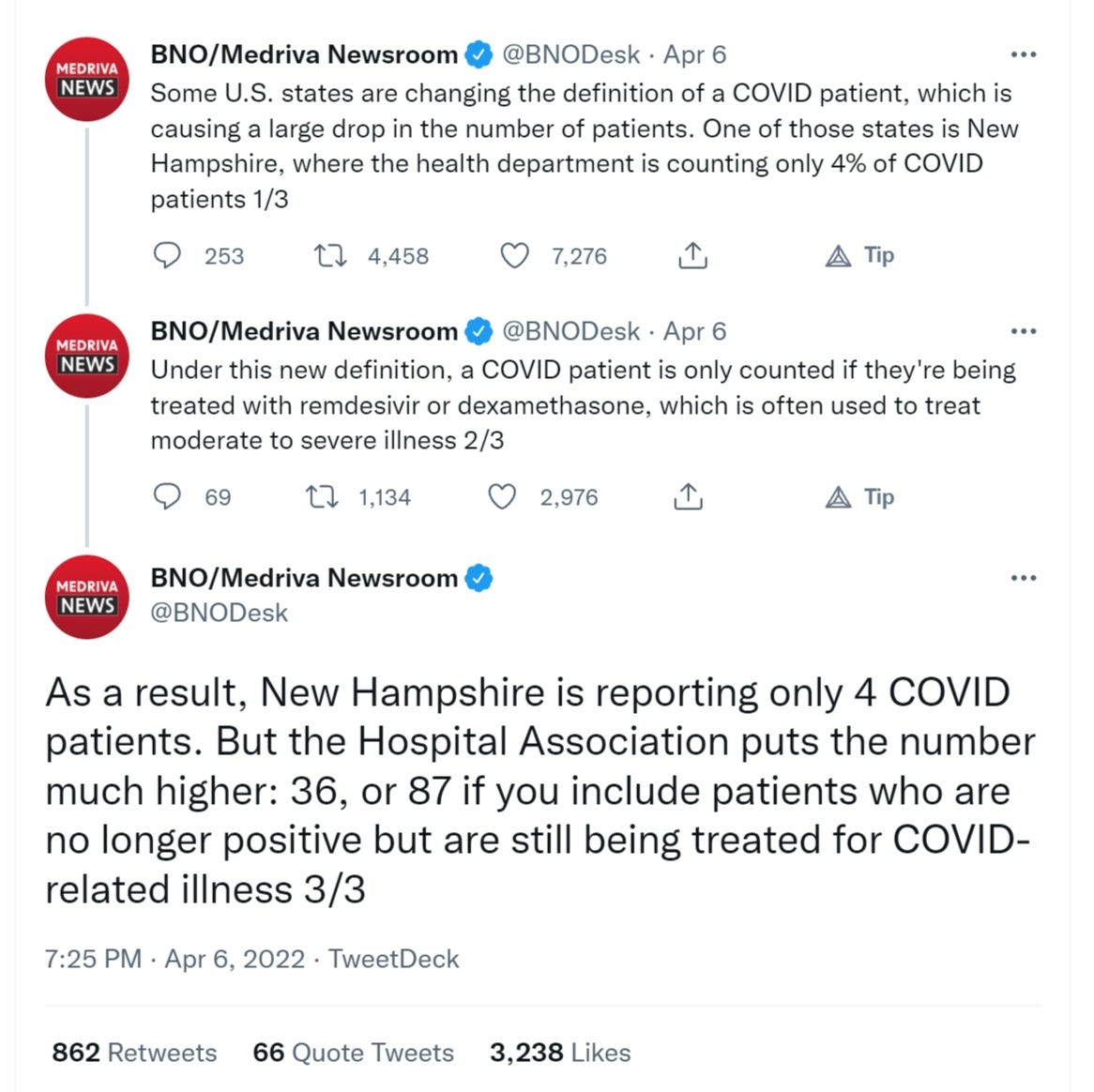
i keep trying to disprove this, but have not been able to thus far and as the US is starting to alter data collection around hospitalization etc, this is going to become increasingly difficult to compare/track domestically. (the cynical might ascribe this to a desire to obscure future waves)
will keep at it.
the truth is in here somewhere.


Comments
Post a Comment